The Migraine World Summit Editorial Team is made up of writers, reviewers, and publishers who carefully review the information provided by our experts, and share those insights in these in-depth articles.
Understanding key medical terminology can be crucial for effective communication, diagnosis, and management of any disease or disorder. Getting a good handle on migraine and headache terminology, with all its complexities, can be especially helpful.
Understanding key medical terminology can be crucial for effective communication, diagnosis, and management of any disease or disorder. Getting a good handle on migraine and headache terminology, with all its complexities, can be especially helpful.
The following guide provides clear, concise definitions for common migraine and headache terms regularly discussed in our Migraine World Summit interviews with the world’s top headache specialists. Peruse this primer, and get a step ahead for the next Summit—and, ultimately, a step ahead in your care.
Types and Classifications of Migraine
Migraine
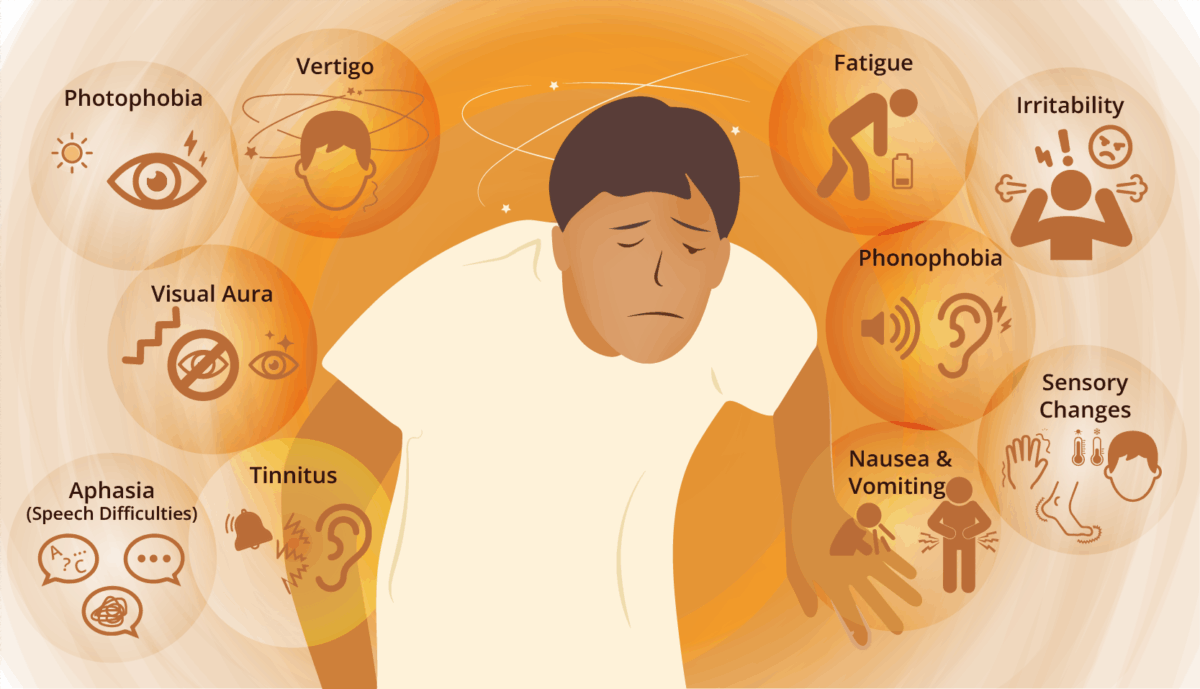
This complex neurological disease is characterized by a severe headache accompanied by other symptoms such as:
This refers to migraine that occurs on fewer than 15 headache days per month.
Chronic Migraine
Chronic migraine is diagnosed when a person experiences headache on 15 or more days per month, for at least three months, with at least eight of those days meeting the criteria for a migraine attack.
This is when an individual has 10-14 migraine attacks per month. While not yet classified as chronic migraine, people with high-frequency episodic migraine are at an increased risk of progressing to chronic migraine.
Migraine with Aura
This is a subtype of migraine that includes transient neurological symptoms that typically precede, or sometimes accompany, the head pain.
Aura symptoms may include: visual disturbances, numbness, weakness, and trouble with language.
This is a severe migraine attack lasting longer than 72 hours. Unresponsive to standard acute treatments, it often requires urgent medical intervention.
It may also be referred to as intractable migraine, which is often used more broadly in clinical settings to describe chronic migraine that is highly resistant to multiple treatments (see refractory migraine), while status migrainosus is the acute, prolonged attack.
Refractory Migraine
This term is used to describe migraine that has not adequately responded to multiple acute and preventive treatments, including oral medications, injectable therapies, and the use of neuromodulation devices.
Managing refractory migraine often involves a multidisciplinary approach.
Hemiplegic Migraine
This is a rare and severe form of migraine with aura that includes temporary motor weakness or paralysis on one side of the body, mimicking stroke symptoms.
It can be familial (FHM) or sporadic (SHM).
Headache Classifications
Primary Headache
This is a headache that is not caused by another underlying medical condition.
A few examples of primary headache are migraine, tension-type headache, and cluster headache.
Secondary Headache
This headache is a symptom of another condition. These conditions can range from minor issues, like dehydration, to serious underlying causes, such as a brain tumor, aneurysm, or infection.
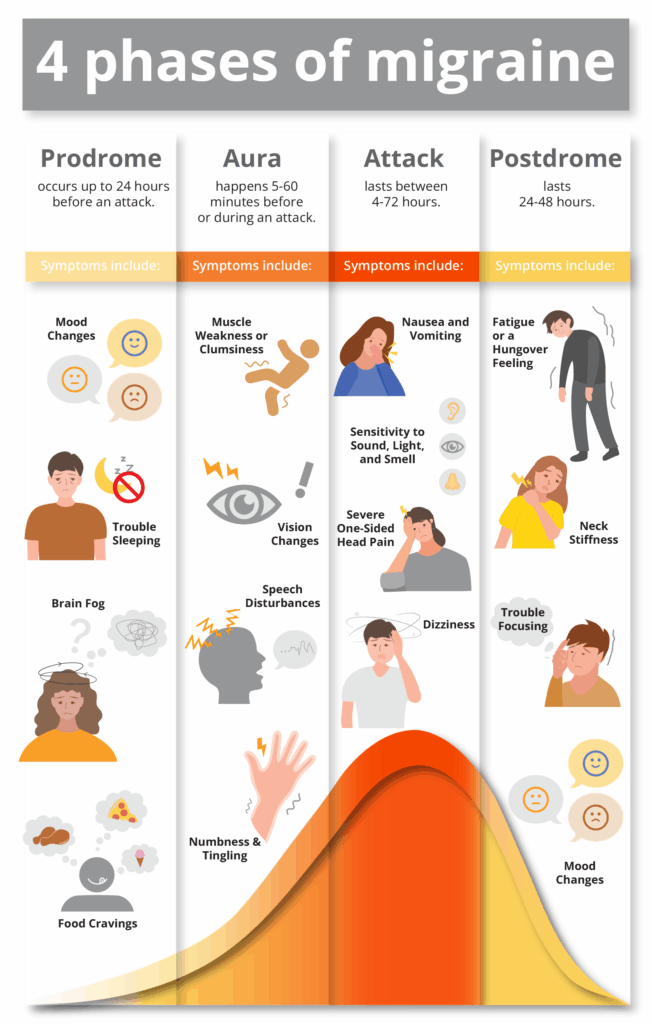
A migraine attack typically progresses through four phases, though not everyone experiences all of them. This article explains the phases in depth.
Prodrome (Pre-headache)
This is the earliest phase, occurring hours or even days before the head pain begins.
Symptoms can include fatigue, mood changes, neck stiffness, food cravings, frequent yawning, and increased urination.
Aura
This phase involves transient neurological symptoms that typically precede or accompany the head pain. Symptoms usually last 5 to 60 minutes and can include:
Visual disturbances (flashing lights or zigzag lines, or blind spots)
Sensory numbness or tingling
Motor weakness
Speech disturbances
Attack (Headache Phase/Ictal Phase)
This is often the most painful phase, characterized by head pain, often throbbing, and usually on one side of the head.
It is commonly accompanied by light sensitivity, sound sensitivity, nausea, and vomiting.
Postdrome (Post-headache)
Following the attack phase, many individuals experience a “migraine hangover.”
Symptoms can include fatigue, difficulty concentrating, mood changes, and neck stiffness.
Interictal
This phase refers to the period between migraine attacks when a person is not experiencing migraine headache.
However, there may still be non-headache symptoms in between attacks such as brain fog, allodynia, or residual sensitivity to sound and light, for example.
Specific Headache Types
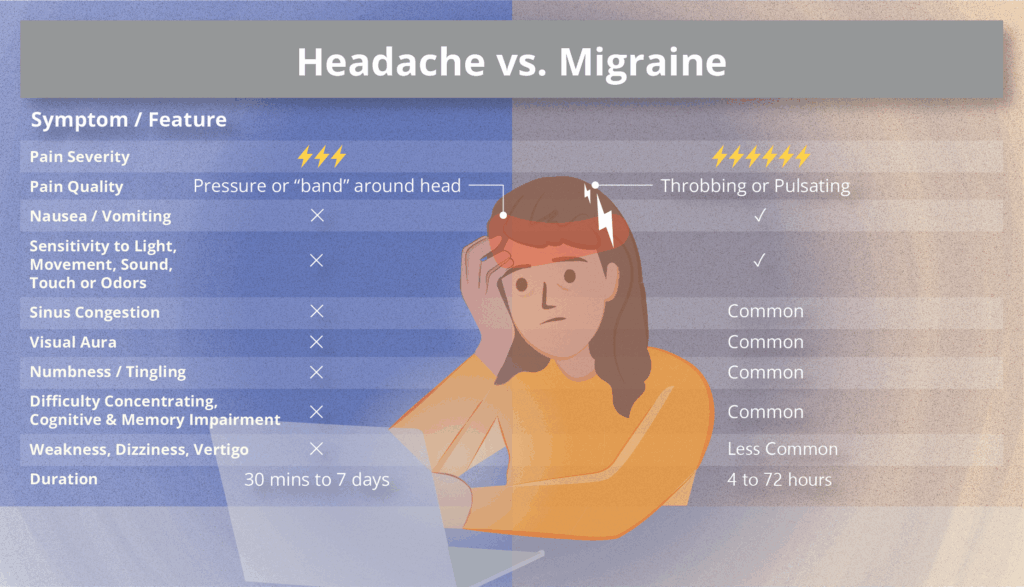
Tension-type Headache
This is the most common type of headache, characterized by mild to moderate pain that feels like a tight band around the head.
It typically lacks the associated symptoms of migraine, such as light and/or sound sensitivity, or nausea.
Cluster Headache
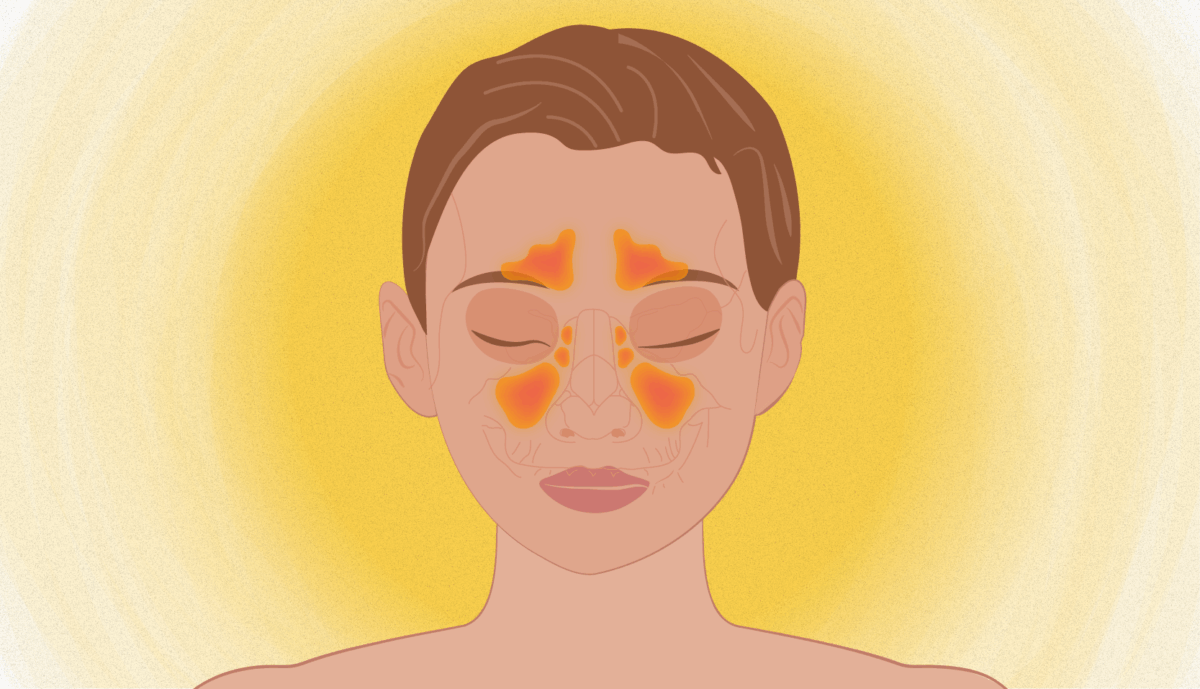
This severe primary headache disorder is characterized by excruciating pain, usually around one eye or temple.
It is accompanied by autonomic symptoms such as tearing, nasal congestion, eyelid drooping, or facial sweating on the same side as the pain.
Attacks occur in clusters, lasting weeks or months, followed by periods of remission.
New Daily Persistent Headache (NDPH)
This is a rare primary headache disorder characterized by a sudden onset of continuous daily headache that does not remit.
The pain is present every day from onset and can have features of both migraine and tension-type headache.
Hemicrania Continua
This is a rare, chronic, unilateral headache that is continuous and fluctuating in intensity.
It is characterized by autonomic features (like tearing or nasal congestion) on the affected side.
It is notably responsive to indomethacin.
Idiopathic Intracranial Hypertension (IIH)
Characterized by increased pressure around the brain, this condition does not have an identifiable cause.
Symptoms often include a daily headache, visual disturbances, and pulsatile tinnitus (hearing rhythmic sounds that match one’s heartbeat).
Medication Overuse Headache (MOH)
This chronic daily headache is caused by the overuse of acute headache medications.
It often occurs when acute medications are taken frequently (e.g., more than 10-15 days per month), leading to a cycle of pain and medication use.
This term is used for medications that are taken at the onset of a migraine attack to stop or reduce the severity of the pain and associated symptoms.
Examples include: NSAIDs, triptans, gepants, and ditans.
Preventive Treatment
This includes medication or therapies taken regularly to reduce the frequency, duration, and severity of migraine attacks.
These are typically considered for individuals with frequent or disabling migraine.
Options may include: beta blockers, tricyclic antidepressants, anti-seizure drugs, Botox, CGRP inhibitors, and more.
Rescue Treatment
These are medications or therapies used when acute treatments have failed to provide relief, or for severe attacks that require stronger intervention.
Sometimes these are provided in an emergency setting.
Key Terms in Migraine Pathophysiology & Symptomatology
Calcitonin Gene-Related Peptide (CGRP)
This neuropeptide is widely distributed in the nervous system, playing a significant role in migraine pathophysiology.
During a migraine attack, CGRP is released from nerve endings, contributing to inflammation and pain signaling.
CGRP Monoclonal Antibodies (mAbs): These are injectable medications used for migraine prevention. They work by targeting either the CGRP molecule itself or its receptor, thereby blocking its pain-promoting effects.
Examples: erenumab (Aimovig), fremanezumab (Ajovy), galcanezumab (Emgality), and eptinezumab (Vyepti).
CGRP Small-Molecule Receptor Antagonists (Gepants): These are oral tablets used for both acute migraine relief and prevention. They block the CGRP receptor, preventing CGRP from binding and activating pain pathways.
Examples: ubrogepant (Ubrelvy), rimegepant (Nurtec ODT), and atogepant (Qulipta).
Allodynia
A condition where a normally non-painful stimulus (like light touch, the brushing of hair, or wearing of glasses) is perceived as painful.
It is a common symptom in migraine, indicating central sensitization (a chronic pain condition in which the central nervous system becomes hypersensitive, amplifying pain signals).
Aura
See “migraine with aura” above.
Brain Fog
A common cognitive symptom experienced by many people with migraine, characterized by difficulty with concentration, memory, and clear thinking.
It can occur during any phase of a migraine attack, including the prodrome and postdrome phases.
Behavioral Treatment
Non-pharmacological therapies that teach individuals skills to manage migraine symptoms and reduce their impact.
Examples include: cognitive behavioral therapy (CBT), biofeedback, and relaxation techniques.
Lifestyle Changes
Modifications to daily habits that can help manage migraine.
These often include maintaining a consistent sleep schedule, regularly exercising, managing stress, identifying and avoiding triggers, and maintaining a healthy diet and adequate hydration.
Neuromodulation
This is the alteration of nerve activity through targeted delivery of electrical or chemical stimuli to specific neurological sites.
In migraine, this often involves non-invasive devices that stimulate nerves like the trigeminal or vagus nerve to reduce pain and frequency.
Nonsteroidal Anti-inflammatory Drugs (NSAIDs)
A class of medications used to reduce pain, fever, and inflammation.
Common over-the-counter (OTC) NSAIDs include ibuprofen and naproxen, often used for acute migraine relief.
Trigeminal Nerve
This is a cranial nerve that provides sensory input from the face and controls the muscles used for chewing (i.e., forehead, cheeks, and jaw).
Phonophobia
This is increased sensitivity to sound, a common symptom during a migraine attack.
Photophobia
This is increased sensitivity to light, a hallmark symptom of migraine, where even normal light levels can be painful or irritating.
Vagus Nerve
A cranial nerve that regulates involuntary bodily functions (i.e., heart rate, digestion, and breathing) and connects the brain to many organs, making it a major part of the parasympathetic (“rest and digest”) system.
While it’s not exhaustive, familiarizing yourself with this list of key terms is an important step in understanding migraine disease. This knowledge can enhance communication with your healthcare providers and contribute to more informed discussions about your care. We encourage you to continue learning through our expert interviews, articles, and additional resources available on the Migraine World Summit website. Make sure to save the date for the next free Migraine World Summit: March 11-18, 2026!
People with migraine are often unsure about whether drinking alcoholic beverages will increase their likelihood for a migraine attack. Many researchers and healthcare professionals have updated their advice in this area based on current research and data. This article shares the latest recommendations from various experts in the migraine field. Ultimately, a person with migraine should consider multiple factors and know how certain key factors in alcoholic beverages play a role in their own migraine disease.
People with migraine are often unsure about whether drinking alcoholic beverages will increase their likelihood for a migraine attack. Many researchers and healthcare professionals have updated their advice in this area based on current research and data. This article shares the latest recommendations from various experts in the migraine field. Ultimately, a person with migraine should consider multiple factors and know how certain key factors in alcoholic beverages play a role in their own migraine disease.
Alcohol’s Complex Relationship to Migraine
Alcoholic beverages have been widely considered by migraine patients and healthcare professionals to play a role in triggering migraine attacks. As far back as 25 B.C., wine was mentioned by Celsus, a Roman scholar, who described “pain” after drinking wine.1 Based on retrospective studies, up to one-third of people with migraine have reported that alcoholic drinks trigger migraine attacks for them.2However, this correlation is not as clear as the medical community once believed.
In fact, recent studies evaluating a link between alcohol and migraine attacks have been inconclusive in establishing this direct correlation. Some researchers even go so far as to conclude that the role of alcohol as a trigger may have been overestimated in the past.3As alcohol use varies greatly between cultures, regions, religions, and individuals, this has made research somewhat contradictory, and the understanding of alcohol’s impact complex.4
Migraine Basics
Migraine is a neurological (related to the brain) disorder, often described as head pain that can be accompanied by symptoms such as light sensitivity, nausea and vomiting, dizziness, stomach pain, brain fog, and much more. Together, these symptoms form what medical providers call a migraine “attack,” which can interfere with a person’s daily activities and significantly disrupt their way of life.
A migraine attack can also be characterized by its phases, which begin before the head pain starts (prodrome), and continue even after the pain has disappeared (postdrome). Patients can have either episodic migraine or chronic migraine. Migraine is more than just a headache and is a disorder that is influenced by genetic predispositions and environmental factors. Patients with migraine often know their personal triggers, i.e., something that happens to them or something they do, which can occur before an attack begins.5
Alcohol’s Effects on the Body
To understand this complex issue it is helpful to understand the effects of alcohol on the body. When a person — with or without a history of migraine — drinks alcohol, many parts of the body are affected as the body processes the alcohol and responds to its compounds.
Neurotransmitters
Alcohol affects chemicals that naturally occur in the brain called neurotransmitters. These neurotransmitters like dopamine, GABA, glutamate, and serotonin allow neurons to communicate with each other, and allow the brain to perform many functions in the body.
“Short-term alcohol consumption depresses brain function by altering the balance between inhibitory and excitatory neurotransmission … Specifically, alcohol can act as a depressant, by increasing inhibitory neurotransmission, by decreasing excitatory neurotransmission, or through a combination of both. Alcohol’s depressant effect on neurons may be associated with some of the behavioral manifestations of intoxication: Alcohol consumption is initially accompanied by decreased attention, alterations in memory, mood changes, and drowsiness (Draski and Deitrich 1995). Alcohol’s excitatory actions (e.g., reduction of social inhibitions) appear to be caused, at least in part, by suppression of inhibitory neurotransmitter systems (Pohorecky 1977).”6
Blood Vessel Changes
Alcohol initially causes blood vessels to expand, increasing blood flow to the brain. However, after long-term use of alcohol, a person can experience high blood pressure.7Changes in the blood vessels are believed to be one of many factors that contribute to a migraine attack but not the direct cause of the attack.
Dehydration
Alcohol consumption causes the body to remove fluids quicker than usual through urinating more frequently. This can lead to dehydration. Dehydration is known to contribute to migraine attacks.8
Inflammation and Blood Sugar
Alcohol can trigger inflammation in the body, which can cause poor appetite, brain fog, and a generally ill feeling. In addition, alcoholic drinks can irritate the lining of the stomach, cause blood sugar levels to fall, and can prevent restful sleep.9
Sleep
For people with migraine, sleep plays a powerful role in migraine management. Whether it is a trigger, a treatment, or a symptom, migraine and sleep impact one another.10Alcohol has a significant impact on sleep. Initially, it may have a sedating effect at the beginning of sleep; though, it also produces poor sleep in the second half of the night.11More information on migraine and sleep is covered in-depth here.
Alcohol Use Disorder/Intoxication
If alcohol is ingested in large quantities it can produce alcohol intoxication, which can be harmful. This can produce alcohol-related symptoms like slurred speech, loss of coordination, and behavioral or emotional changes.
Alcohol dependence, also known as alcoholism, is a chronic disease that causes a person to crave alcohol, produces an inability to stop drinking, and causes withdrawal symptoms when the person tries to stop.12
Chronic alcoholism can also cause brain and liver damage. As the liver regenerates from the chronic stress of alcohol exposure, it builds scar tissue. This scar tissue prevents the liver from filtering fluids properly and, therefore, toxins that are normally excreted by the liver are released into the body. This can lead to alcohol encephalopathy, similar to early dementia, and also ascites, which is fluid pooling in the abdomen. The liver also filters the blood in the body. When this is disrupted by a strained liver, the blood can pool in veins and rupture, which in turn can cause internal bleeding or even death.13
Seeking Help
In the US: If you or someone you know is in need of assistance for alcohol use disorder, please seek medical advice; and/or if you need help finding the right treatment option, please visit alcohol treatment.niaaa.nih.gov.14
Alcoholic drinks have compounds in addition to the alcohol (ethanol) itself that can trigger migraine attacks in some people. These are components like phenols, flavonoid radicals, histamine, sulfites, tyramine, and tannins, which all have the potential to be migraine triggers.
Not only do alcoholic beverages have histamine, but they can also cause the body to release histamine. The release of histamine has been identified to be a migraine attack contributor.15
Sulfites are chemicals used as preservatives for food, beverages and medications, preventing them from going “bad.” They are frequently used to slow browning and discoloration (caused by bacterial growth) in foods and drinks. Sulfites can also occur naturally in some foods and beverages. Sulfites are found in virtually all alcoholic drinks including wine, beer, ciders, and liquor. Winemakers have used sulfites for centuries to preserve the color and flavor of wines, especially red wine. There are no alcoholic drinks that are truly “sulfite free,” though there are companies that reduce the amount of added sulfites. For some migraine patients choosing low-sulfite wines can be helpful, and also choosing high-quality brands or spirits.16,17
Tyramineis another compound that occurs naturally in some beverages and foods like aged, cured, fermented, and leftover foods. Tyramine is produced during the aging or fermentation process. Some people with migraine report symptoms when exposed to these foods. It is important to remember that tyramine doesn’t affect everyone equally.18
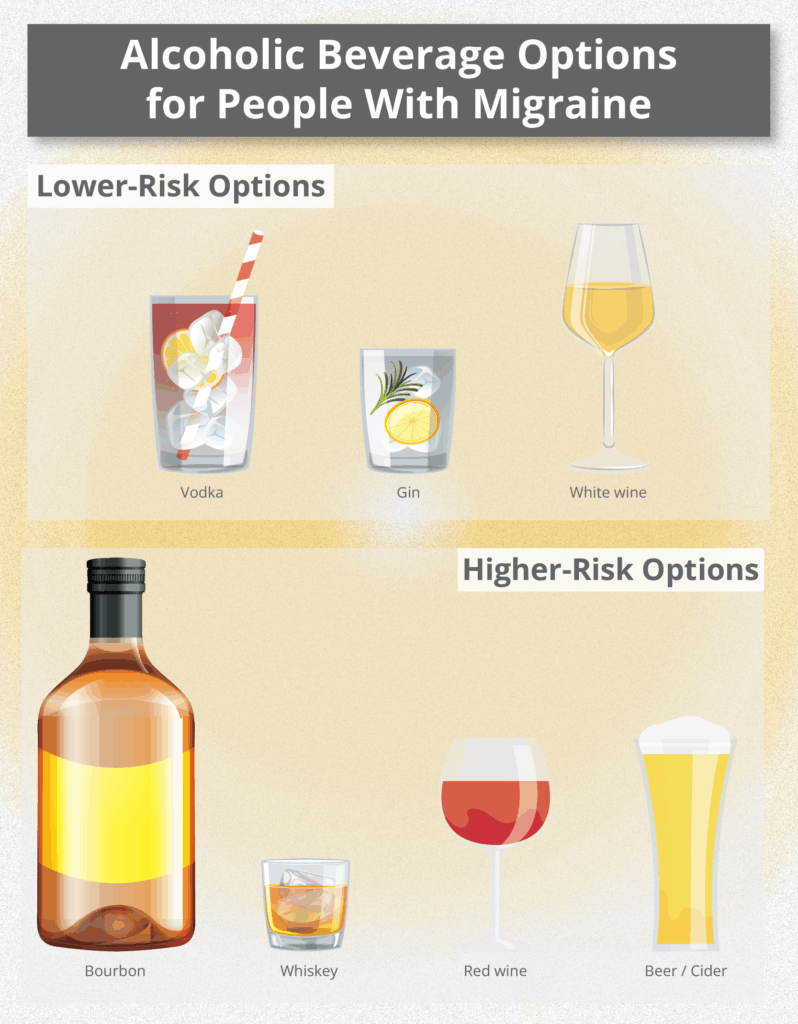
Additionally there are compounds known as congeners, which are byproducts of fermentation and add to the taste and smell of drinks.19 Examples of congeners are tannins, ketones, acids, and esters. Drinks that are low in congeners are often clear or colorless like vodka, white wine, sake and gin. Alcoholic beverages that have high congeners are darker in color like whiskey, cognac, red wine, and rum.20 It is believed that drinks that are high in congeners have a higher risk of producing a migraine attack for some people.
Below are a few alcohol options that tend to fall on the higher-risk side or lower-risk side for most people with migraine; note, however, that differences vary per person and can even vary from day to day for one person, depending on other potential triggers. After all, some triggers, like those that are environmental (i.e., barometric pressure changes) or hormonal (i.e., the start of a menstrual cycle) are often out of a person’s control.
Carl Cincinnato and Dr. Paul Mathew, assistant professor of neurology at Harvard Medical School, discussed “Alcohol and Migraine” at the 2023 Migraine World Summit.
In this clip from the 2023 Migraine World Summit, Dr. Paul Mathew discusses “Alcohol and Migraine.”
Does Alcohol Trigger Migraine Attacks?
It is important to consider the difference between alcohol-induced migraine and delayed alcohol-induced headache (DAIH). For people with migraine, if there is a headache after drinking alcohol, they may assume the alcohol triggered a migraine attack. Patients with migraine can also experience a hangover headache, which is different from a migraine attack. See below to compare the two types.
Alcohol-Induced Migraine vs. Delayed Alcohol-Induced Headache (DAIH or Hangover Headache)21,22
smaller amounts of alcohol than that of non-migraine people
moderate to excessive amounts of alcohol
Common Symptoms
throbbing or drilling pain; nausea; vomiting; sensitivity to light, sound, and smell; low mood; neck pain
throbbing or pulsating head pain (worse with physical activity), dizziness, diarrhea, fatigue, nausea
Location of Head Pain
often unilateral
usually bilateral
Intensity
mild to severe
moderate
Also, there are many variables that can trigger a migraine attack. Common triggers can include everything from poor sleep to weather changes, stress, and hormone fluctuations. It is challenging to isolate these triggers to determine which are influential factors.
“It’s kind of dangerous to take any single trigger in isolation. So, for example, I’ll give you a ridiculous example: A patient will have a slice of pizza and say, ‘Oh my God, I had a migraine. I’m never eating pizza again!’ When they completely forget that they didn’t sleep all the night before, they’re under tremendous stress from a new job, there are seasonal fluctuations, there [are] hormonal fluctuations going on.”
Dr. Mathew shares, “So, really, it’s not good practice to just look at a single trigger and say, ‘Well, this is what I’m going to modify,’ and kind of ignore everything else. Alcohol is very much the same way, as well. I often tell patients that everybody’s response to different forms of alcohol will be different, and it’s no different than food.”23
Many people with migraine disease keep a diary or log, on paper or their phone, to identify suspected triggers. Apps like Migraine Buddy make it simple. Triggers for migraine are varied and individual. Dr. Starling from the Mayo Clinic talks about the benefits of keeping a diary or log and understanding triggers in the context of migraine.
In this clip from the 2017 Migraine World Summit, Dr. Amaal Starling discusses the importance of migraine-related tracking.
It is also important to acknowledge that it is often the combination of triggers that cause an attack and not just one. For some patients, one alcoholic drink will consistently cause a migraine attack; for others, it is a drink plus other triggers that precipitate an attack. For many, alcohol can be a trigger one day, and not on the next.
People with migraine should also consider how much alcohol they are consuming and the type of alcohol they drink as factors affecting their risk for an attack. Migraine attack provocation is very individual and not universal. A diary to identify the effects of alcohol on a migraine attack can be helpful.
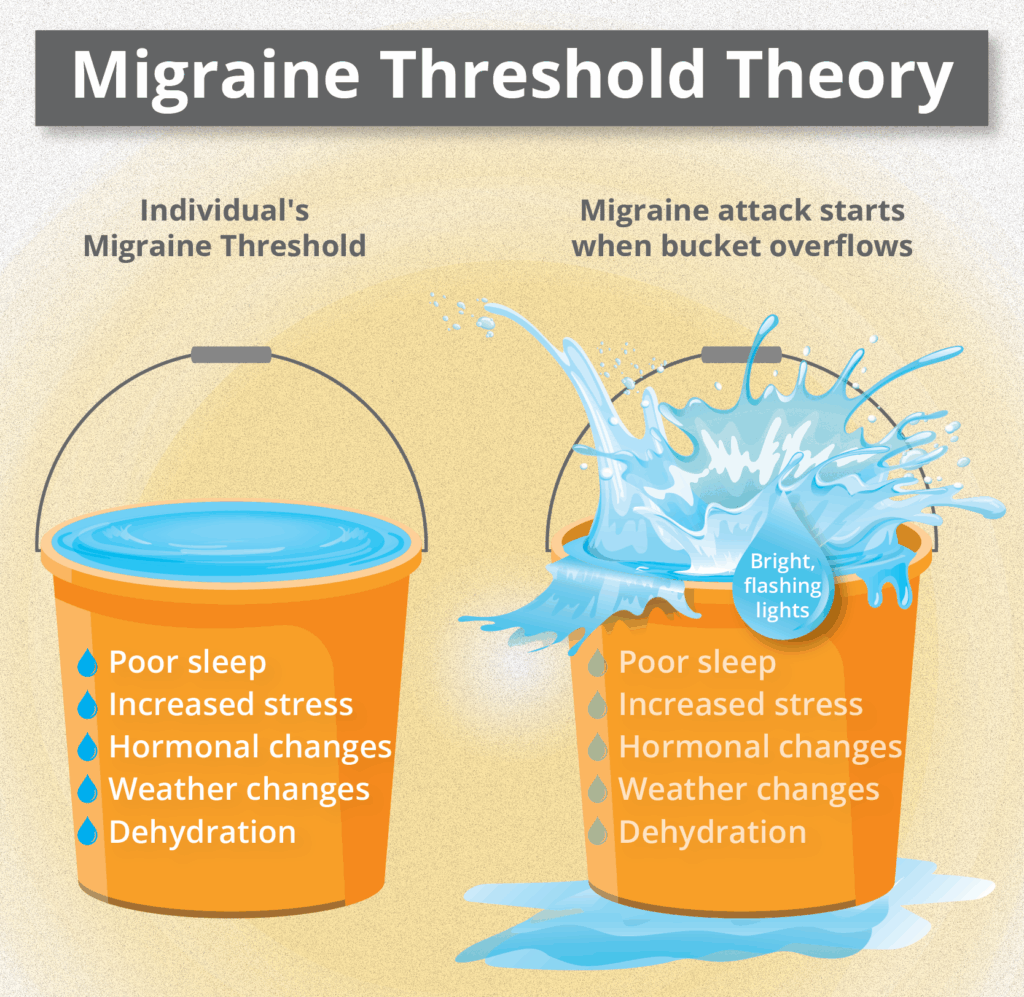
Threshold Theory for Migraine
When learning about migraine, patients are often introduced to the “migraine threshold” concept and how it can affect the likelihood of an attack. Migraine triggers are often cumulative, meaning they add up over a certain period of time. An individual’s threshold can change, and the type of trigger can vary over the course of the disease as well. Watch or listen to Dr. Catherine Stark describe what migraine threshold is and how it can help people understand the effects of triggers on their migraine disease.
Dr. Catherine Stark discusses “What Causes Migraine and Its Symptoms” at the 2021 Migraine World Summit.
As Dr. Stark illustrates, a person’s migraine threshold changes from day to day because certain triggers are going to be out of one’s control. For example, Mother Nature doesn’t listen to someone telling her not to send a thunderstorm. The migraine threshold is individual for each person and, therefore, can be reached with different triggers than those of other people with migraine. It is helpful for individuals with migraine to prioritize some of the lifestyle basics, like sleep and hydration, in order to prevent their threshold from being crossed.
Migraine Treatment Options When Drinking Alcohol
When treating migraine after consuming alcohol it is important to be cautious of any medications that are processed through the liver. A common over-the-counter pain reliever that many patients use for migraine symptoms is acetaminophen, or Tylenol. Acetaminophen is processed through the liver and can be toxic to the liver if taken in large quantities and combined with alcohol. Healthcare providers encourage patients who are consuming larger quantities of alcohol to avoid using acetaminophen.
The use of NSAIDS, non-steroidal anti-inflammatory drugs like ibuprofen (i.e., Advil, Motrin), are also used for migraine treatment and should also be used carefully when combined with alcohol. Triptans, like rizatriptan and sumatriptan, are considered safe options when treating migraine and consuming alcohol. 24
Rehydrating the body after consuming alcohol can be helpful in treating migraine attacks. One of the best ways to avoid having symptoms while drinking is to keep adequately hydrated. Alcohol is a diuretic, which causes the body to lose fluids faster than usual through urination. Staying hydrated while drinking may help prevent dehydration and, therefore, prevent migraine symptoms.25
Experts say that if you are experiencing vomiting or diarrhea from either excessive alcohol intake or a migraine attack, then electrolyte drinks can be helpful. However, migraine patients should be mindful of other ingredients in these products such as colorants and artificial sugars, which can be triggers for some.26
Tips for Reducing Trigger Risk When Drinking Alcohol
Lifestyle Basics That Can Be Helpful
Sticking to low-glycemic foods
Not skipping meals
Proper hydration
Healthy sleep habits
Decreasing stress
Exercising
Additional Tips
Drink alcohol with food.
Drink responsibly, and know one’s limits.
Limit the total amount of alcohol.
Know how certain types of alcohol affect one’s body.
Track symptoms after drinking different types of alcohol.
Keep hydrated with water, or alternate water with alcohol.
Drink slowly.
Consider one’s threshold, and the cumulative triggers at that time.
Non-Alcoholic Alternatives for People With Migraine
Mocktails — great for social events
Herbal teas
Sparkling sodas
Non-alcoholic or de-alcoholized beer or wine
Water or sparkling water
Summary
Migraine disease and triggers vary from person to person. Alcoholic drinks are problematic for some people living with migraine and not for others. When determining if alcohol is a trigger, it is important to consider the type of alcohol, the ingredients of an alcoholic drink, and the person’s experience with these beverages. Planning ahead and knowing one’s own migraine experience with alcohol can help one decide if drinking alcohol is feasible for them.
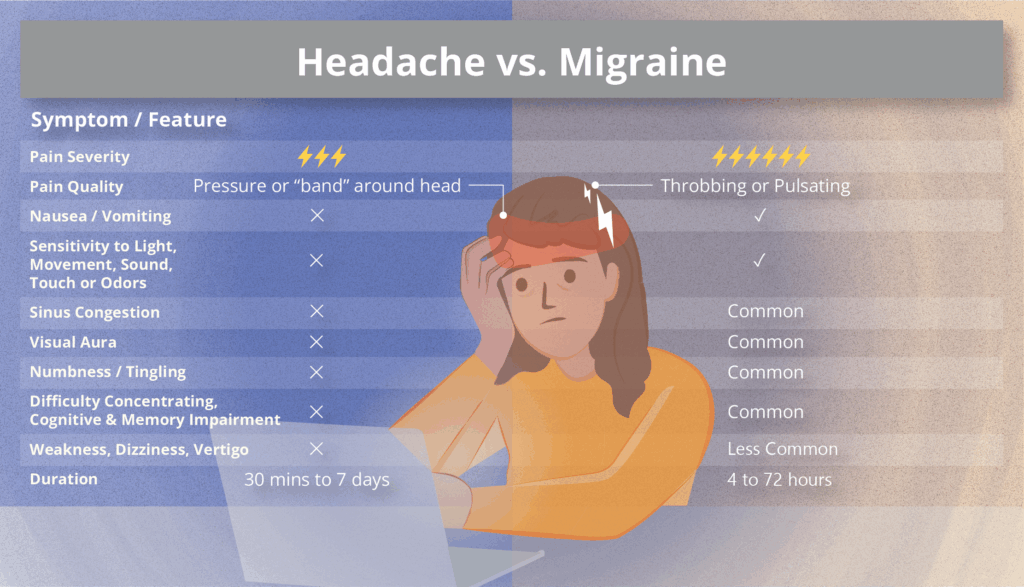
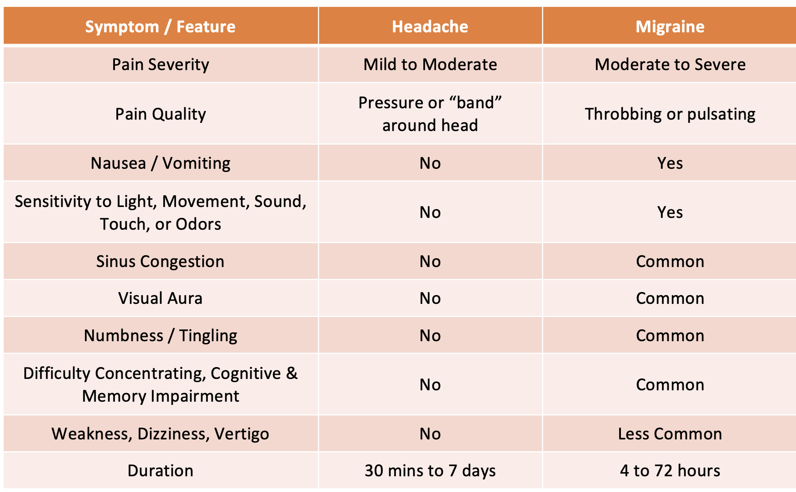
Although many people believe that migraine is simply a bad headache, this is a widespread misconception. Migraine is, in fact, a neurological disease where headache is one of the symptoms.
Although many people believe that migraine is simply a bad headache, this is a widespread misconception.
Migraine is, in fact, a neurological disease where headache is one of the symptoms.
In addition, people with migraine can suffer from a long list of ailments, which may include:
Nausea and vomiting,
Neck pain and muscle aches,
Sensitivity to light, sound and scents,
Fatigue,
Dizziness or vertigo,
Numbness or tingling,
Visual disturbances, such as a temporary visual aura (which can include flashing lights, zig-zag lines,or other visual changes) and/or persistent visual phenomena (ongoing visual disturbances beyond the aura phase of a migraine attack),
Cognitive issues such as brain fog, having trouble finding the right words, difficulty concentrating, and mood swings.
A migraine attack can affect systems throughout the body. This combination of physical and mental symptoms helps explain how a migraine attack can profoundly disrupt daily life.
Dr. Olivia Begasse de Dhaem, a neurologist and headache specialist who advocates for people living and working with migraine, shares how this disease can impact people’s lives very differently.5
She says that migraine affects people in different ways, and even one person can have different symptoms or varying presentations of the disease throughout their life. So, even within the same person, migraine is not always the same. Another element is the interaction between the disease and other factors of a person’s lifestyle, like the type of job functions they perform, their work hours, and work environment.
Why Migraine is a Significant Workplace Issue
Migraine affects over a billion people worldwide.8 One of the reasons why migraine is such a common condition in the workplace is that its peak intensity occurs in peoples’ 20s and lasts until their 40s.7
In fact, migraine is the leading cause of disability among young women. As many as one in four women aged 35 to 55 struggles with migraine during what should be the prime years of her career and family life.2
Even with acute and preventive therapies, migraine still disrupts the lives of 90% of those affected, impacting many parts of their lives, including work, cognitive function, and emotional health.4
Migraine is also a widely underdiagnosed and undertreated condition, with its severity often underestimated by healthcare professionals.9Studies show that 45% of people with migraine hesitate to seek medical care, and 42% of those who hesitate never sought migraine care.18
Impact of Migraine at Work
Absenteeism vs. Presenteeism
When examining the impact of migraine in the workplace, we distinguish between absenteeism and presenteeism.
Absenteeism is when a person is absent from work because of migraine.
As many as 90% of those living with migraine say that they are not able to work fully during a migraine attack.19 Studies show that people living with migraine miss an average of 4.4 more workdays per year than those without the condition.16
Presenteeism, or functional impairment, refers to when a person with migraine experiences an attack during work hours and continues to work, but with reduced productivity. They are functionally impaired. The vast majority of migraine-related productivity loss is due to presenteeism.6 On average, people living with migraine experience reduced productivity on 11.4 workdays each year.16
“Eighty-nine percent of migraine-related productivity loss is due to presenteeism. So, people come and are present at work, but they’re not as productive as they normally would be because of all the symptoms of the disease.”
When experiencing a migraine attack, people are about 50% as effective as they are normally.5 This is explained to be due to the head pain and other symptoms, the unpredictability of the attacks, comorbidities, and emotional impact. On top of being underdiagnosed and poorly managed, migraine also carries a stigma that affects people living with the condition.
Studies show that even on non-headache days, migraine can negatively impact work productivity as well.6 About 40% of people living with migraine have symptoms, such as trouble with focusing, decision-making, thinking quickly, and remembering things, in between their migraine attacks. In addition, cogniphobia, the fear that mental exertion might trigger another migraine attack, may interfere with work productivity as well.6
Global Epidemiology and Impact (prevalence, direct and indirect costs)
As mentioned, migraine is a widespread condition, impacting roughly 14-15% of people around the world.1 More than 1 in 7 employees live with migraine,14 and according to The 2019 Global Burden of Disease Study, migraine is the second leading cause of disability worldwide,2 more common than asthma, diabetes and epilepsy combined.3
According to Dr. Begasse de Dhaem, the workforce includes a diverse mix of individuals living with both episodic and chronic migraine. She also says that approximately 46% of those with low-frequency migraine are able to work full time, whereas only 35% of individuals with chronic migraine manage to maintain full-time employment.
When it comes to the direct and indirect costs of migraine in the workplace, it is difficult to pinpoint a clear or definitive number. This is particularly true given that 89% of migraine-related productivity loss is due to presenteeism, and currently, there are no standardized methods for measuring presenteeism.6
That said, several studies estimate that the cost of presenteeism in the workplace is 3-10 times higher than the cost of absenteeism due to migraine.6
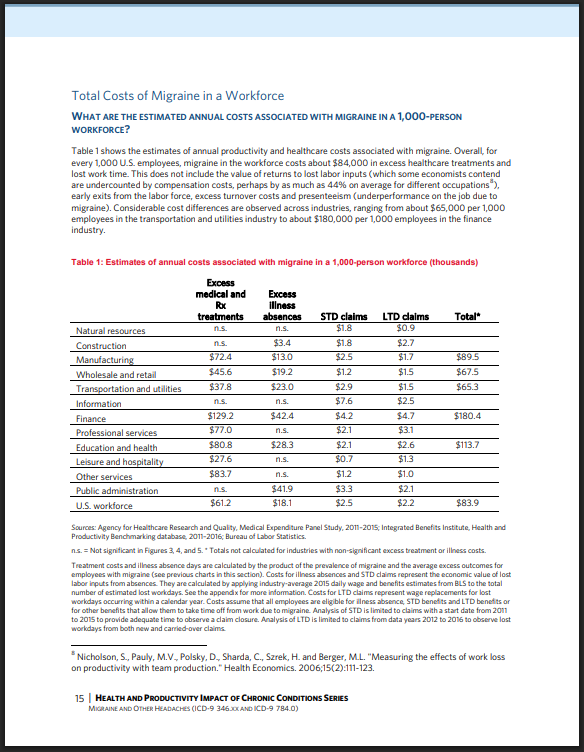
According to estimates from the Integrated Benefits Institute, for every 1,000 U.S. employees, migraine costs approximately $84,000 in excess healthcare expenses and lost work time.10 This figure does not include lost labor input, early exits from the workforce, excess turnover costs, or the impact of presenteeism.10
In the report «The Health and Productivity Impact of Chronic Conditions Report: Migraine and Other Headaches», Integrated Benefits Institute shows the financial burden across different industries due to medical treatments, absences, and disability claims.11
In the U.K., a report from the Work Foundation estimates that migraine costs the economy £8.8 billion per year in lost productivity.11 The same report also states that approximately 86 million workdays are lost annually due to migraine, and that close to £1 billion is spent on healthcare costs due to migraine.11
A European study called Eurolight found that migraines cost the EU economy around €27 billion each year in lost productivity.15 Most of this loss happens because employees don’t perform as well at work, or because they quit their jobs, mainly because they don’t get the support they need.
In addition, there is a huge personal cost for people living with migraine. The burden of migraine-related disability and productivity loss due to the disease can negatively impact a person’s career choices, job status or security, financial situation, workplace relationships, mood, and self-confidence.6
How Migraine Attacks Can Be Triggered At Work
For individuals living with migraine, the work environment can contain several triggers that may increase the risk of an attack. Being mindful of these factors can help reduce the frequency and severity of episodes.
Common workplace-related triggers include the following:17
High or inconsistent stress: Sudden changes in workload, high pressure, or the feeling of lack of control
Bright lights: Especially fluorescent lights or glare from screens
Excessive screen use: Long periods in front of a computer without breaks
Unsociable work hours or shift work, which can cause irregular sleep patterns
Loud noises or constant background noise from people, machinery, etc.
Poor diet: Skipping meals or irregular eating habits
Bad posture: Prolonged sitting in non-ergonomic positions that cause tension in the neck and shoulders
Sharp smells or fragrances: i.e., strong perfumes, cleaning agents, or industrial odors
Recognizing and addressing these triggers, both individually and at the organizational level, can help create a more supportive and inclusive work environment for employees with migraine.
When talking about triggers, it is important to recognize that there is often an excessive focus on migraine triggers, even among healthcare professionals. A person living with migraine can do their best to avoid or manage known triggers, and still get migraine attacks. Migraine is a neurological disorder characterized by recurring attacks that are often caused by things outside of one’s control, such as unforeseen stress, weather changes, and hormonal shifts.
When asked at the 2021 Migraine World Summit what type of work might be best suited for those living with frequent or chronic migraine, Melanie Whetzel, lead consultant of the cognitive/neurological team at the Job Accommodation Network (JAN), replies: “We can’t tell people with migraine — or any disability — what the best job is for them, but we recommend focusing on key concerns. If lighting is an issue, avoid large offices or retail spaces, and opt for a private office, cubicle with adjusted lighting, or remote work. If fragrances are a trigger, avoid florists, department stores, or malls with scented products. For noise sensitivity, consider noise-canceling headsets, earbuds, or soundproofing panels. The main point: Identify and avoid work environments that worsen migraine.”13
What People With Migraine Worry About In The Workplace
Juggling work and the unpredictability of living with migraine can often lead to a hidden burden that goes far beyond physical symptoms. Many worry about job security. They fear that their frequent absences or reduced productivity may put their employment at risk or limit opportunities for promotion and career advancement.
“The thing I hear the most commonly in my practice when seeing patients is a fear of being fired or having to quit the job because of all of the symptoms of the disease, but also because of the stigma.”
In a survey of over 200,000 U.S. workers, only 22% of them found migraine to be a serious enough reason to miss work.6 Because of this, many may also struggle with the decision of whether to disclose their diagnosis, unsure of how it will be received.
Lack of understanding from colleagues and managers can add to the stress of the disease itself. Many feel guilty or even ashamed when an attack affects their ability to contribute, and they may avoid speaking openly about their condition out of fear of being stigmatized or seen as unreliable.
According to Whetzel, the fact that migraine is an unseen disability can make navigating the workplace especially challenging.13
Whetzel says: “If somebody’s lost an arm, and they come into work, I think people kind of have an idea of what they might be able to do, and what they might have difficulty with. But for someone with migraine — if you don’t have migraine, if you don’t have someone in your family with migraine — then it might be more difficult for you to really think about, ‘OK, what really are the issues?’ ”
This emotional strain, combined with the neurological impact of the condition, can lead to lower self-confidence, increased stress, and a sense of isolation. Addressing these concerns requires not only awareness, but also a supportive and flexible work environment that takes invisible illnesses seriously.
Coping With Migraine Stigma At Work
Migraine stigma is everywhere, coming from coworkers, family, friends, doctors, as well as institutions such as health insurance agencies and the media; and it can be internalized. In fact, studies show that there is more stigma against chronic migraine than any against other neurological disease.5
In a survey of 2,000 people in the U.S. who didn’t have migraine themselves but knew someone who did, many had negative views:6
39% said people with migraine tend to hide their condition.
35% believed the attacks were caused by the person’s own unhealthy habits.
32% thought people with migraine exaggerated their symptoms.
31% believed migraine was used as an excuse to get out of work or school.
29% felt they made things harder for their coworkers.
Because of this kind of stigma, more than half of workers who stay home due to migraine keep the reason to themselves.6
This often makes it harder for people with migraine to do their best at work. When people feel that work is difficult because of their migraine, they also tend to report more disability and worse impact, when filling out the Migraine Disability Assessment (MIDAS) scale.6
“I think most people hide their migraine at work. And I think taking a step back, it’s not necessarily that they want to hide it, but migraine is highly stigmatized. It’s the most stigmatized of the neurological diseases — stigmatized at work, in language, institutions, in medicine — I mean it’s stigmatized everywhere. So as a result to people, you kind of internalize stigma and self-stigmatize and that sometimes, subconsciously and involuntarily, leads to concealment.”
Dr. Begasse de Dhaem believes that an important way to fight stigma is by talking openly about migraine and helping others understand what it really is.
She explains, “When people with migraine share their experiences, it helps others see that they’re not so different; they just face extra challenges, especially at work. Explaining the condition can lead to more understanding, more support, and less judgment. Of course, not everyone feels safe opening up, especially in a toxic work environment where there’s a fear of being treated unfairly or even fired. It takes courage to speak up, and not everyone can or should do it. But for those who can, being open can help the whole migraine community. It can also lead to feeling more seen, heard, and appreciated.”
She adds, “… living and working with migraine is hard, and people deserve recognition for showing up and doing their best despite the pain.”
Rob Music, chief executive of The Migraine Trust London, talks about the importance of patient advocacy and how it can be done. The video is from the 2024 Migraine World Summit.
Disclosure and Communication
What Employers Need to Know About Migraine
If you are an employer who has employees living with migraine, it is important that you acknowledge that this neurological disease is so much more than just a bad headache. The unpredictable nature of migraine makes it challenging for employees to manage without support and flexibility, and the stigma surrounding migraine often leads to it being underestimated.
By fostering a more informed and supportive workplace culture, employers can reduce stigma and help employees with migraine feel safe and valued. When people feel understood and supported, they’re more likely to stay in their jobs and do their best work.
It is also important for employers to recognize that people living with migraine often develop valuable qualities that can benefit any workplace.15
Carl Cincinnato, executive director at Migraine at Work, explains in a recent webinar on Navigating Migraine in the Workplace: Strategies for Success: “As they learn to balance work with a chronic health condition, skills like flexibility, endurance, empathy, time management, and problem-solving are sharpened through navigating daily challenges. As a result, people with migraine can be highly resourceful, committed, and collaborative. Some of your most talented and resilient team members may, in fact, be those living with migraine.”17
Pros and Cons of Disclosing Your Migraine at Work
Speaking openly about migraine at work can have both significant advantages and potential drawbacks.
On the positive side, being open about your condition can make it easier to request accommodations and create a more supportive work environment. It may also allow you to qualify for legal protections, and provide greater job security by helping protect against unfair dismissal. Sharing your experience can also build a sense of community and offer support to others, while allowing you to be your authentic self and feel more accepted.
However, there are also drawbacks to consider. Disclosure might lead to fewer career opportunities, reduced privacy regarding your health, and the risk of being seen as overly sensitive or even being labelled a hypochondriac.
Weighing these pros and cons is important when deciding whether to speak up about migraine in the workplace.
“Disclosing migraine at work can help reduce stigma through greater understanding and education. It is a really hard and brave thing to do that can benefit the wider community. But whether or not to share depends on the work environment, and it’s completely valid not to disclose if the setting feels unsafe or unsupportive.”
When and How to Talk to Your Employer
Deciding whether to talk to your employer about migraine can feel overwhelming, but in some situations, it can make a real difference. Opening up may lead to better support, more understanding, and practical changes that improve your daily work life.
Here are some signs that it might be the right time to start the conversation:15
If migraine is affecting your performance at work or getting worse
If reasonable accommodations could make a big difference
If you need help from HR to challenge a denied health or leave benefit
If you are a care partner of a family member who is struggling with migraine
If you want to see the work environment and culture become more supportive and help others who may be struggling
Telling your workplace that you live with migraine isn’t always easy, especially in environments where stigma still exists. That’s why it helps to prepare. Think about what you want to say, what support you need, and how migraine affects your job.
It can help to talk about it with your doctor or someone you trust. Try to find allies at work or in support groups. If you can involve your supervisor, they might be able to make small changes that help a lot.
Dr. Begasse de Dhaem advises, “It’s important to stay true to yourself, and do what feels right for you. Many people with migraine carry guilt, often because of stigma, and feel like they always have to push through. But do you really have to attend that late work event? How does your body feel? Sometimes it’s OK to say ‘no.’ Others might simply say, ‘We missed you,’ and move on. Society teaches us to push through pain, but it’s worth pausing to ask: ‘What do I really need right now?’—not what I feel I should do.”
Katie MacDonald, director of Operations Miles for Migraine, talks about migraine advocacy. She urges you to explain your symptoms — not just say ‘I have a migraine.’ This way you can help others understand the reality of the disease and break the stigma. The video is from the 2024 Migraine World Summit.
Rights and Legal Protections
What Counts as a Reasonable Accommodation
According to Melanie Whetzel with JAN, simple, low-cost accommodations can make a big difference for employees living with migraine.13
“Most of the accommodations for individuals of migraine are inexpensive; either they don’t cost anything at all, such as, you know, creating a space for individuals to lie down, or they’re under $500. So it’s really, really inexpensive to create changes that can have a huge impact.”
Frequently requested options include:
flexible scheduling
working from home
lighting adjustments
noise adjustments
fragrance-free workspaces
access to quiet spaces
“It’s important to talk with the person to understand their work conditions and what’s realistically possible. The key is to adjust based on the individual’s needs and environment,” says Dr. Begasse de Dhaem.
If you’re afraid to ask for accommodations at work, a doctor or headache specialist can be a helpful ally. They can write a letter of support or communicate with HR on your behalf, often without disclosing the specific diagnosis.5 This protects your privacy while still explaining that you have a serious health condition and need support.
Talking with healthcare providers, support groups, or even a social worker can help you feel more prepared and confident to ask for the adjustments you’re legally entitled to.5
Whetzel encourages employers and employees to experiment with short-term adjustments to see what works.13
“We often recommend temporary or trial accommodations. Working from home is a good one to try on a trial basis, because the employer is not locked into anything. With a trial period, an employee can show the employer if they can work from home and be as productive,” Whetzel explains.
Snapshot of Protections for People Living with Migraine
Many countries have laws that protect people with disabilities from unfair treatment at work. While the wording may differ, the core principles are similar: If your disability significantly affects your ability to do daily tasks or job functions, you may be entitled to reasonable accommodations and protection from discrimination.
Here’s a quick look at some of the disability acts from different countries:
Stacey Worthy, an expert in workplace law and health policy, explains how the Americans with Disabilities Act (ADA) applies to people living with migraine.
Worthy says, “The way the ADA works, it’s all on a case-by-case basis, so there’s not a list of conditions that automatically qualify as disabilities. Instead, you have to meet that definition of disability of an impairment that substantially limits one or more major life activities which, for many individuals with migraine, they absolutely meet that definition.”
In the video clip below, Worthy explains in more detail when these protections apply to someone living with migraine — and under what circumstances they might not.
Stacey Worthy explains in detail the Americans with Disabilities Act and how it applies to people living with migraine. The video is from the 2019 Migraine World Summit.
Can You Get Fired Because of Migraine?
Many people living with migraine worry that disclosing their condition at work could cost them a promotion, or even their job, during the next round of layoffs. But is that actually legal?
According to legal expert Stacey Worthy, the answer is: “It depends, but generally, no.”12
Employers are not allowed to fire someone because of a disability like migraine. However, they can let someone go for reasons unrelated to the condition, such as a company-wide layoff.
Worthy says, “They’re also allowed to let you go if your condition could pose a direct threat to your health or safety or the health and safety of someone else. So, let’s say you have migraine with aura, which is creating a visual impairment, and you’re a truck driver. That could potentially be a direct threat to the health and safety of yourself and others, because you could potentially get into an accident.” She adds, “And then the other instance is if you’re unable to perform the essential functions of your position, they could potentially let you go for that reason as well.”
Tips for Managing Migraine at Work
Managing migraine at work isn’t always easy, but small changes can make a big difference. Whether you’re working from home or in the office, these practical tips can help reduce triggers, ease symptoms, and support your overall well-being throughout the workday.
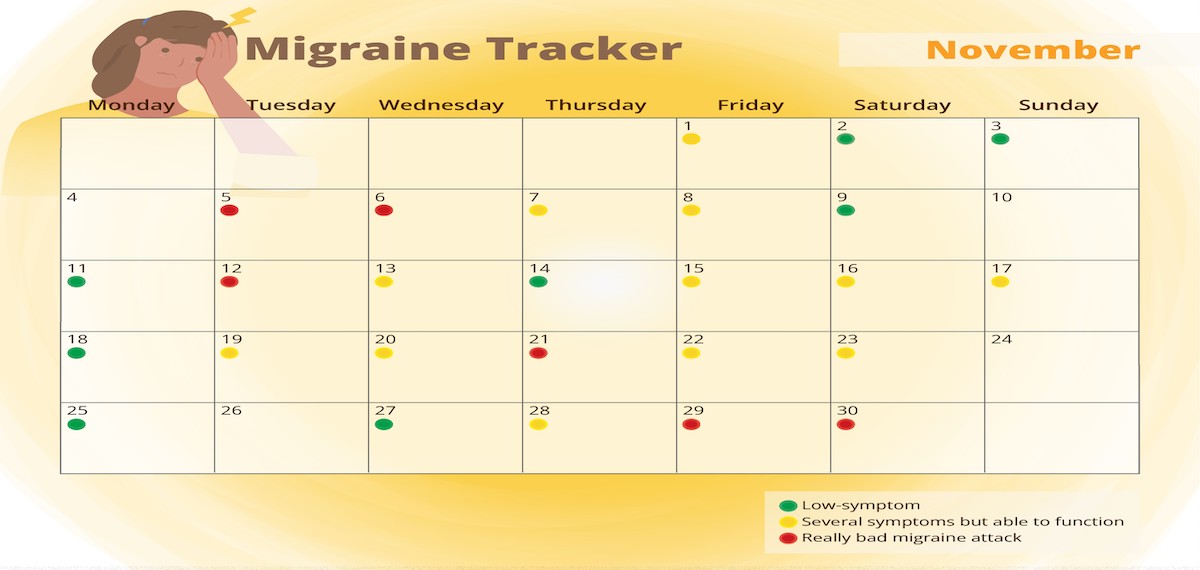
Keeping a Journal and Identifying Triggers: Tracking your symptoms, environment, stress levels, and diet can help you identify patterns over time. While not all migraine attacks can be prevented, understanding how your body responds allows you to manage triggers more effectively and lessen the overall impact on your daily life.
Utilizing a migraine management tool kit: Keep essential items at your desk or in your bag — like medication, sunglasses, a water bottle, earplugs, or snacks. Having what you need nearby can help you act quickly when symptoms begin.
Taking micro pauses: Regular, mindful breaks throughout the day, while stretching or focusing on your breath, can reduce muscle tension and eye strain.
Find a coworker who can be your advocate: As we all know, a migraine attack can come on all of a sudden and progress quickly. That is why it may be helpful to know someone has your back if you’re unable to speak for yourself at the moment. Find a colleague you trust who can support you during an attack or help explain your needs to others.
Lifestyle modifications: Stick to a consistent routine with meals, caffeine, hydration, and sleep. Small lifestyle changes can reduce migraine frequency and make workdays more manageable.
Want to learn more? In this article you can read more about migraine and sleep.
Supportive Workplace Culture
What Employers Can Do Better for Employees With Migraine
In addition to what you previously read about accommodations, employers will benefit from building a migraine-friendly workplace.
People with migraine tend to be more productive at work when they feel satisfied in their job, have support from their manager, work in a positive environment, and have some control over how they do their tasks.6
One way to do this is to initiate a migraine workplace program. If the whole company learns about migraine, including those who don’t have it, the pressure to explain the condition over and over falls away from the people living with the condition. And as a big bonus, studies show that such programs cut absences due to migraine, increasing productivity during an attack, and decrease the costs due to migraine-related productivity loss.6
Migraine Workplace Programs
Migraine workplace programs are useful to educate employers and employees, which again can result in better understanding and a more compassionate work environment.
Such workplace programs usually follow three simple steps:6
Teach all employees about migraine through a company-wide awareness campaign.
Offer a voluntary and private way for employees to check if they might have migraine disease.
Give those who are diagnosed the option to join a support program or get connected with treatment.
According to six prospective cohort studies in the U.S., workplace migraine education programs have shown great results:6
Boosted productivity from 2% to 36%,
Reduced sick days by 25%,
Cut down the number of days people worked while having a migraine by 32%,
Helped people get about 10% more done during migraine attacks,
Lowered stigma surrounding the condition.
Case Studies
One standout example is the Fujitsu Headache Project, developed in partnership with the Japanese Headache Society and the International Headache Society’s Global Patient Advocacy Coalition.6
Through a combination of e-learning, workplace exercises, and virtual headache consultations, the program reached over 73,000 employees in Japan, making it one of the largest workplace migraine initiatives to date.
The results were impressive:
95% of employees completed the one-hour e-learning module.
After the course, nearly 73% reported that their understanding and attitude toward migraine had changed.
The percentage of employees who viewed migraine as a serious disease rose from 47% to 71%.
Over 77% said their attitude toward coworkers living with migraine had become more supportive.
The program also included a virtual consultation service with headache specialists. Although only a small percentage (0.5%) of employees opted in, more than half of those who received consultations went on to visit a headache clinic and start treatment.
One notable example involved a woman with chronic migraine who had previously endured significant symptoms in silence. After beginning treatment, the impact of migraine on her quality of life dropped to just 10–20% of what it had been, and her productivity at work greatly improved. Her colleagues celebrated her recovery as a workplace success.
The program also introduced headache exercises as part of daily self-care routines, including neck stretches and tension-relief techniques, which were well received. The overall goal was not only to improve quality of life and productivity, but to create a workplace where people with migraine felt safe, understood, and empowered to seek care.
Fujitsu’s initiative has since become a global model for corporate migraine support and has been recognized by the International Headache Society’s Global Patient Advocacy Coalition (GPAC) for its leadership in creating a migraine-inclusive work environment.
Conclusion
Key Takeaways
Migraine is one of the most common, and most misunderstood, conditions in the workforce today. It affects not only physical health, but also cognitive function, emotional well-being, job performance, and career development.
In this article you have read about the many ways migraine can challenge people living with the condition, and the real stigma people still face. It also presents, however, promising solutions in forms of education, accommodations, workplace culture change, and legal protections.
Encouragement for Employees and Employers
To employers and managers: You don’t need to be a medical expert to make a meaningful impact. Listening, learning, and offering flexibility goes a long way. Creating a migraine-friendly workplace isn’t just the right thing to do, research suggests that it also will benefit the culture at your workplace and productivity.
It is important to recognize that when employers and employees work together to understand and support those with migraine, everyone benefits.
Chronic migraine is a neurological condition that can severely limit an individual’s quality of life. It can disrupt daily obligations, impacting mental health, and often lead to physical and social challenges.
Chronic migraine is a neurological condition that can severely limit an individual’s quality of life. It can disrupt daily obligations, impacting mental health, and often lead to physical and social challenges.
To understand chronic migraine, it’s important to see how it affects people both physically and emotionally. Living with constant and unpredictable migraine attacks can create ongoing worry and stress, which can sometimes make the symptoms worse.
Through accurate diagnosis, appropriate treatment, and a few lifestyle adjustments, however, people with chronic migraine are often able to manage symptoms and improve their quality of life. This article will cover the essentials of chronic migraine: What it is, how it differs from other headache illnesses, and also what its symptoms, causes, risk factors, and treatment options are.
The goal is to help people with migraine better understand chronic migraine and offer strategies to manage symptoms, thereby reducing its impact on their lives.
Understanding Chronic Migraine
Chronic Migraine Defined
Before discussing the definition of chronic migraine, it helps to define what makes up a migraine attack.
As mentioned, migraine is a neurological condition that involves many symptoms, whereas the head pain often is the most prominent. Other common symptoms include nausea, vomiting, and sensitivity to light (photophobia) and sound (phonophobia).1
A migraine attack often includes moderate to severe headache pain that can last 4-72 hours, if left untreated.1 A typical migraine headache is described as throbbing pain on one side of the head that worsens with physical activity.1 Some people also experience an aura before the migraine, which may include temporary visual or sensory disturbances that gradually disappear.1
In addition to migraine with and without aura, there are additional types of migraine, which may include symptoms like dizziness, abdominal pain, weakness on one side of the body, and more. In this article you can find additional information about the different types of migraine. It is also useful to understand the different phases of migraine attacks.
Chronic migraine is defined by The International Classification of Headache Disorders (ICHD-3) when someone experiences headache on 15 or more days each month, for at least three months; and on at least eight of those days, the headache features typical migraine symptoms.2
This higher frequency of debilitating attacks in chronic migraine can lead to a near-constant state of pain and other migraine symptoms, often turning a person’s life upside down.
How Chronic Migraine Differs From Episodic Migraine
Chronic and episodic migraine are both types of migraine disorders, but they differ mainly in headache frequency and impact. According to The International Classification of Headache Disorders ICHD-3 beta criteria, episodic migraine refers to having less than 15 days a month with head pain and/or other migraine symptoms.3 Episodic migraine attacks occur less frequently and often allow more recovery time.
Pathophysiology of Chronic Migraine
Pathophysiology is the study of what goes wrong in the body to cause a disease or condition. It looks at how normal body processes get disrupted, leading to symptoms.
Although researchers still don’t fully understand what causes chronic migraine or why some people’s migraine attacks progress from episodic to chronic, it is believed that certain factors may play a role. This includes changes in how the brain processes pain, an increase in the brain’s sensitivity, and even structural changes in the brain itself.5
Researchers also believe it’s possible that people with chronic migraine are in a constant “warning phase” before an attack, which might keep these pain-processing changes active and make the brain even more sensitive over time.5 This is also known as central sensitization.
“The more frequently you get pain, the more frequently pain can cause itself. We have studies that show us that patients who have attacks that are frequent can start to have these processes in the brain where the brain is more sensitive, and it’s easier to get that next attack because the brain’s ready,” explains Dr. Jessica Ailani, a clinical professor of neurology at MedStar Georgetown University Hospital in Washington, D.C.
Prevalence & Global Impact of Chronic Migraine
About 14–15% of people worldwide are affected by migraine,6 making it a common condition on a global scale. Chronic migraine is estimated to affect 1-2% of the general population, and about 8% of people living with migraine.7
Did you know?
The 2019 Global Burden of Disease Study found that migraine is the second biggest cause of disability worldwide for both genders and all ages, and the first most common cause of disability among young women.8
Migraine contributes to approximately 4.9% of the global burden of ill health, measured in terms of years lived with disability (YLDs).6
More than one billion people worldwide live with migraine, with the highest prevalence among young adults.9 For most people living with migraine, the peak intensity occurs in their 20s and lasts until their 40s.9 This makes migraine a condition that significantly disrupts what should be some of the most productive years of life, during which individuals typically focus on education, career advancement, and starting families.
Migraine affects both men and women, but it is three times more common in women than men.10 For women, migraine occurrence is often related to changes in hormone levels. Attacks may start around the first menstrual period or arise during pregnancy when hormone levels shift significantly.10
These statistics highlight the significant role migraine plays in worldwide disability and the overall impact on health.
Symptoms & Comorbidities of Chronic Migraine
Common Symptoms of Chronic Migraine
People living with chronic migraine report a whole range of symptoms that often blend together along with the frequent headaches.11 While head pain can be disabling on its own, the additional symptoms can be even more disabling for people with chronic migraine. These include:
Nausea and vomiting
Loss of appetite
Dizziness
Constant sensitivity to light, sound, smells, or movement
Neck pain
Fatigue
Cognitive issues are also common among people with chronic migraine. Many individuals report feelings of brain fog, or just feeling like their brain is moving a little slower than normal. The following symptoms are examples of how this is often illustrated:
Feeling confused
Having trouble finding words
Mood changes
Trouble with concentration
Frequency, Duration & Severity of Attacks
When someone with migraine transitions from episodic to chronic migraine, the nature of their attacks often changes. Instead of having distinct attacks with a clear beginning and ending, people with chronic migraine may experience a continuous blur of head pain and other symptoms, making it difficult to pinpoint when one attack ends and the next begins.
Dr. Christine Lay, a professor of neurology at the University of Toronto and headache specialist who helps people living with chronic migraine every day, explains that this shift occurs because the brain’s pain threshold changes, making attacks easier to trigger even without clear causes.11
According to Dr. Lay, it is important for patients to take note in their migraine diary and talk to their healthcare provider about the days in between where they might not have a lot of head pain but may experience other symptoms.
Dr. Amaal Starling, a neurologist, headache specialist, and associate professor of neurology at the Mayo Clinic College of Medicine, agrees with Dr. Lay, and says that people living with chronic migraine often do not give the whole picture when they talk to their healthcare provider.
Dr. Starling says she asks her patients these two questions to help determine a more accurate diagnosis of chronic migraine:12
How many days per week or per month are you having headache or any migraine symptoms?
How many days per week or per month do you have zero headache or migraine symptoms whatsoever?
Comorbidities to Chronic Migraine
Comorbidities are other health conditions that often occur alongside a primary condition. People living with migraine have a range of comorbidities, the most common being:13
cardiovascular disease (including stroke and heart attack)
depression and anxiety
sleep disorders (including insomnia and restless legs syndrome)
other pain disorders (like fibromyalgia and back pain)
Studies show that these comorbidities are more common in people with chronic migraine than in people with episodic migraine.13
In addition, Dr. Dawn C. Buse, psychologist and clinical professor at Albert Einstein College of Medicine, adds the following comorbidities to being common for people living with migraine:28
epilepsy
multiple sclerosis (MS)
panic disorders
suicidality
nonsuicidal self-injurious behavior
Hoping to squash the stigma, Dr. Buse stresses that people with comorbidities shouldn’t feel bad, guilty or embarrassed because life with migraine is life with comorbidities. She says that if someone doesn’t have any comorbidities, then they are the most rare unicorn, because almost everyone’s going to have them. It has to do with all sorts of genetic predispositions, neurotransmitters, inflammation, things happening systemically in the whole body, as well as external forces, both environmental and social.
It is important to share all your symptoms with the healthcare professional caring for your migraine. Other medical conditions may affect your headache diagnosis. Also, some headache treatments are unsafe or contraindicated in people with certain conditions or who are on certain medications that may have negative interactions.13
Dr. Buse says there is some data that shows that if one of these conditions gets better, the others might as well. They kind of travel together. She advises that it’s a good thing to actively treat as many of your comorbidities as possible — or at least monitor them for safety.
Dr. Rebecca Burch has studied migraine comorbidities as part of her research through Brigham and Women’s Hospital at Harvard Medical School. In this video she explains more about mood disorders that are highly comorbid with migraine. Which comes first, the pain or the depression? The video is from the 2021 Migraine World Summit.
Living with chronic migraine involves much more than just coping with intense and frequent head pain. This condition can significantly reduce the quality of life for those affected, and can often impact a person’s self-esteem and confidence, as people may feel misunderstood or judged by others who don’t fully understand their condition.
Chronic migraine often results in social isolation, as people avoid potential triggers or fear having another attack when away from home. This can lead individuals with migraine to limit their enjoyment of daily activities and engagement with loved ones, hobbies, work, and other meaningful life events, leaving them feeling isolated and disconnected from the world.
The frequency of attacks and time spent in pain and other debilitating symptoms often leads to physical limitations, making exercise and movement challenging. Chronic pain can also disrupt sleep, and together these effects can create a negative cycle and affect one’s overall well-being.
Chronic migraine can also lead to feelings of anxiety, depression, irritability, and emotional exhaustion due to the unpredictable nature of attacks. Cognitive difficulties like brain fog and difficulty concentrating or remembering can be common both during and in between migraine attacks for those living with chronic migraine. This can be especially difficult to deal with in a work setting.
Chronic migraine can also lead to financial stress due to missed workdays, decreased job performance, and healthcare costs for treatment and medications.
Chronic Migraine & Mental Health: When It’s Time To Do Something
The disappointment of failed treatments, guilt from missed commitments, the strain from suffering relationships, and the fear of the next attack are common feelings for someone living with chronic migraine. It’s a burden that is carried on top of a chronic disease that can leave someone feeling isolated and unfairly judged.14
How does one know when their mental health has become a problem that needs to be addressed? This is how Dr. Buse views this question:
… When you feel you’re not living life as you’d like, you might notice it affecting work, school, or a loss of interest in hobbies or social activities. This isn’t just the burden of migraine making things hard to do; it’s feeling like you don’t want to anymore. That’s likely a sign of depression, and it’s worth discussing with a healthcare professional, like your primary care doctor.
Why Some People Develop Chronic Migraine
Common Causes & Risk Factors
Migraine attacks are believed to happen due to a mix of brain sensitivity, genetic factors (most people with migraine have a family history of it), and the body’s reaction to stress or hormonal changes.15 This leaves women particularly vulnerable due to hormonal fluctuations throughout their lives, including puberty, menstruation, pregnancy, and menopause.
Over time, some people with episodic migraine experience an increase in attack frequency, leading to chronic migraine. This transformation can be driven by underlying neurological changes, such as central sensitization, a process where the brain and nervous system become more sensitive to pain signals. For a person living with migraine, this can feel like anything and everything triggers an attack.
This process can be seen as a threshold issue: a combination of predisposing factors and repeated headache episodes gradually lowers the brain’s tolerance for migraine attacks, making the transition to chronic migraine more likely.7
Although the reasons why episodic migraine can turn into chronic migraine are complex, some factors that increase the risk of this progression include:
Obesity 7
Depression7
Asthma12
Sleeping disorders12
Other pain disorders12
Lower educational status7
Stressful life events7
Acute medication overuse7
Ineffective acute treatment7
Dr. Lay explains how this last bullet point can do a lot of damage.
… You often end up doing more harm than good if you’re a patient who says, ‘I don’t want to take any preventive; I’ll just tough it out. And I’ll wait and take my triptan when I’m [having] a red headache, and I’m in bed and sick.’ You’re actually just increasing the burden, and you’re increasing your disability, and we don’t think it’s good for your brain.
Dr. Lay also discusses grappling with taking acute medication early enough while, at the same time, trying to avoid medication overuse headache, further explained below. This video is from the 2022 Migraine World Summit.
Diagnosis and Medical Evaluation
Definition and Diagnostic Criteria (ICHD-3) for Chronic Migraine
The International Headache Society has published a comprehensive classification system that organizes all types of headache disorders in a detailed, hierarchical format. This system serves as a resource for accurate diagnosis and standardized research across headache-related conditions.
To get the diagnosis “chronic migraine” a person needs to fulfill these criteria set by the International Classification of Headache Disorders (ICHD-3):2
A: You have headaches that feel like migraine or tension-type headache on at least 15 days per month for over 3 months, and fulfill criteria B and C.
B: You have had at least five previous attacks, meeting the standard criteria for migraine (either with or without aura), and fulfilling criteria B-D for 1.1 Migraine without aura and/or criteria B and C for 1.2 Migraine with aura.
C: On at least 8 days each month, for more than 3 months, you have headache that meets any of the following:
Feels like migraine when the attacks start and is relieved by medications like triptans or ergot derivatives.
D: Not better accounted for by another ICHD-3 diagnosis.
Conditions That Can Present Like Chronic Migraine
Certain conditions share symptoms with chronic migraine, making accurate diagnosis challenging. Status migraine, also called status migrainosus, is a debilitating migraine attack that lasts for more than 72 hours.16
Another similar condition is medication overuse headache (MOH). This is also often called rebound headache, and typically occurs when someone takes acute pain medications more frequently than recommended over a period of three months or longer.17
Studies from various countries show that more than half of individuals experiencing headaches 15 or more days per month have MOH.18 Clinical observations reveal that most patients with MOH see an improvement in their symptoms after stopping the overuse of medication, which also enhances their response to preventive treatments.18
High-frequency episodic migraine (HFEM) refers to experiencing 8-14 migraine attacks per month. While this term is not yet an official classification in the International Headache Society’s system, it is gaining recognition in headache research and clinical practice.27
New daily persistent headache (NDPH) is a type of chronic daily headache that can be similar to chronic migraine. This headache does not build up over time, but starts suddenly and becomes a chronic daily headache right from start.4 People usually remember the exact day it started. The pain can feel like a migraine attack, a tension-type headache, or even a mix of both, but it does not have any defining features that make it easy to classify as one or the other.4
Importance of Accurate Diagnosis
Since chronic migraine can often resemble other headache disorders, a thorough evaluation by a healthcare provider is critical. Getting an accurate diagnosis is key to managing chronic migraine and improving a person’s quality of life. It helps a healthcare provider understand which treatment options are best suited for their patient.
Without a precise diagnosis, patients may receive treatments that don’t address the underlying issues, potentially leading to unnecessary side effects or even worsening their symptoms.
Role of Neurologist/Headache Specialist
Primary care physicians are often the first to diagnose and treat people living with migraine. They may prescribe migraine medications, recommend lifestyle changes, and refer patients to specialists if needed.
While finding a headache specialist can be challenging due to their limited availability, neurologists are often a helpful alternative since they frequently treat migraine patients. Not all neurologists specialize in headache, but many are experienced in diagnosing and managing migraine disorder, making them a valuable resource for those struggling to find effective relief.
The Role of Lifestyle in Chronic Migraine Management
Lifestyle changes are proven to help reduce migraine.12 The SEEDS approach, recommended by experts like Dr. Starling,22 focuses on:
Consistent sleep routines, regular exercise (starting small if necessary), balanced meals, and staying hydrated can all help reduce migraine frequency and severity.
There’s no universal migraine diet because triggers vary between individuals. It is helpful, however, for people living with migraine to recognize personal patterns when it comes to food and beverage, rather than follow a strict diet.21 When it comes to stress management, the goal isn’t necessarily to eliminate stress entirely, but techniques like mindfulness, biofeedback, and relaxation can empower individuals to cope more effectively.22
Medical Treatment Options for Chronic Migraine
Preventive Medications for Migraine
Preventive medication for migraine comes in various options, but all have the same purpose: To reduce how often a person gets migraine attacks and reduce the impact that migraine has on their life, or ideally, both.
First-line treatment options for migraine prevention include:
Anti-seizure medication
Blood pressure-lowering medication, including beta blockers and calcium channel blockers
Other approved treatments for migraine prevention include:17
Antidepressants
Gepants
Calcitonin Gene Related Peptides (CGRP) monoclonal antibodies (mAbs)
OnabotulinumtoxinA(Botox)
For people living with chronic migraine it might take time to find the right preventive medication. Many also experience that they need to use more than one preventive medication to get an adequate effect. A combination of preventive medications may have a positive synergistic effect.23
The American Headache Society (AHS) has released an updated consensus statement advocating for the use of calcitonin gene-related peptide (CGRP)-targeting therapies in migraine prevention. They encourage that these treatments should be considered first-line options alongside with today’s approved first-line preventive medications, without the necessity of trying and failing other treatment classes first.29
Finding the Right Treatment for Chronic Migraine
When someone is living with chronic migraine, it is essential to have a treatment plan that addresses both immediate migraine relief and long-term prevention. Different types of over-the-counter and prescription medications, both acute and preventive, can complement each other effectively. Lifestyle alterations can also have a significant impact.
According to Dr. Lay, there are definitely alterations in the structure of the brain due to chronic migraine. It’s not fully understood why this happens or what’s going on in the body and brain to cause it, but she says they do know it is possible to change it.
We don’t really fully understand how or why, but we do know that doing all the right things, such as lifestyle factors, [nutritional supplements], getting out for a walk, mindfulness, meditation, treating your attacks when they come, getting on top of them early, and looking at preventive therapy, are all really important to reverse from chronic migraine to episodic migraine, but also to reverse some of those brain changes.
Non-Drug Approaches to Chronic Migraine Management
In addition to migraine medication, newer treatments suggest that alternative approaches, like complementary and integrative therapies, can aid in migraine attack prophylaxis and help reduce the disability that often comes with chronic migraine.25 This can make a big difference for people dealing with the daily impact of migraine.
These options range from biobehavioral therapy, which includes techniques like biofeedback, mindfulness, and cognitive behavioral therapy (CBT), to acupuncture, shown to help reduce migraine frequency when done consistently.25 Studies are showing about 8-10 sessions are needed to determine if acupuncture is helpful in reducing migraine frequency. And these are usually twice a week.25
Physical therapycan address contributing factors like neck tension or TMJ,25 while neuromodulation devices target nerve activity to alleviate or prevent attacks.
Emerging treatments likebrain retraining focus on rewiring brain pathways to manage chronic pain. Dr. Bethany Ranes, a cognitive neuroscientist, whose field bridges neuroscience and psychology, explains what happens by doing brain retraining.
“Brain retraining works by focusing on the pathways, or connections, in our brain that control our bodies. These pathways are like roads that brain cells use to communicate and interact.“We used to think these pathways were fixed, especially after childhood. But new technology has shown us that we can change them, even as adults.”
Dr. Ranes talks about the “Boulder Back Pain” study that is used as evidence that brain retraining, specifically pain reprocessing therapy, is an effective strategy for treating chronic pain. The video is from the 2022 Migraine World Summit.
Developing a Personalized Migraine Action Plan
Coping with Migraine Stigma
A common stigma surrounding migraine is that it’s “just a bad headache” that’s easy to fix. Many people with migraine fear being seen as weak and lazy, or that it’s “all in their head,” or even that they’re faking it.
Dr. Robert Shapiro, a professor of neurological sciences at the University of Vermont, explains one excellent way to combat the stigma.
“The method that has been reported to have the most effectiveness is what’s called ‘contact.’ Contact is, quite simply, someone who carries a stigmatizing attitude interacting directly with somebody who is stigmatized.”
He reiterates, “So educating yourself about the disease is really a helpful thing, so that you can explain to others what you’re experiencing.”
For people living with migraine it can be useful to keep a migraine diary to keep track of migraine attacks and symptoms, medications used, and medication effects.
Many people with migraine have a tendency to only keep track of the very bad days, but it is also very important to keep track of days with milder head pain, as well as days affected by other symptoms.
Dr. Lay explains, “There are a number of different symptoms that go along with that head pain: feeling confused, having trouble finding words, the light, sound, and smells that are bothering you, your clothing bothering you, feeling like you’ve lost your appetite, frank nausea, even vomiting. So, what I encourage my patients to do is to keep track of the headache because that’s sort of the first clinical sign that a migraine is underway for many of us. So, you must write down those headache days. But I do have patients track other days, as well. And I want them to make note of crystal-clear days and, a truly migraine-free day, not just a headache-free day, but a migraine-free day.”
Collaborating with Healthcare Providers
Working closely with healthcare providers is essential for the effective treatment of chronic migraine. By openly sharing one’s symptoms, triggers, and any changes in their condition, a patient can help their provider understand their unique needs and tailor a treatment plan accordingly.
Regular check-ins allow for adjustments to medication, lifestyle recommendations, and preventive strategies. Building a strong partnership with one’s healthcare team can lead to better outcomes, as the practitioner can support the patient in finding the most effective ways to manage and reduce migraine attacks over time.
Creating an Emergency Kit for Migraine Attacks
When managing chronic migraine, a person may have more migraine days than the number of days they are recommended to use acute medications. For this reason, it can be helpful to have an “emergency kit” with alternative options to offer support on migraine days.
What to put in the kit is up to the individual. It depends on what their biggest migraine triggers or symptoms tend to be. Maybe a person is really sensitive to light and sound, or maybe it’s nausea that is the most disabling. Others find that a hot or cold compress can help provide distraction from pain and reduce inflammation. Avoiding dehydration is also important. That said, here are a few examples of what to include in the kit:
Acute medication — medication that helps stop an attack once it’s started
Sunglasses, migraine glasses, or an eye mask — to help with light sensitivity
Earplugs or noise-canceling headphones — to help with sound sensitivity
Cold or warm compresses — to help relieve inflammation and distract from the pain
A water bottle and electrolytes powder — to assist in staying hydrated
A migraine cooling/menthol stick/roll-on — to help soothe attacks with a cooling sensation
A neuromodulation device — modulates nerve activity to block pain signals, helping to prevent or stop attacks
A Reliefband — relieves nausea through emitting pulses that stimulate the median nerve, normalizing the nerve messaging from the brain to the stomach
Self Care Strategies
Coping mechanisms and self care are vital tools for managing the challenges of chronic migraine. By practicing self kindness rather than self stigmatizing, or blaming oneself for an attack by thinking, “I stayed out too late” or “I didn’t take care of myself,” is essential to hold onto.
Acceptance also plays a big role for people living with migraine. Acknowledging that migraine is a neurological, biological disorder, and that it is not the person’s fault that they get migraine attacks, may allow the person to shift their energy toward proactive management, rather than self blame, and work to improve their quality of life.
Practicing self care also means listening to one’s body’s needs, such as resting during a migraine episode. Identifying and setting boundaries, both in personal and professional settings, can help prevent overexertion, which may worsen symptoms.
Support Systems
Seeking emotional support through friends, family, or support groups can provide a sense of community and reduce feelings of isolation. A good support system can affect a person’s quality of life a great deal.
Dr. Lay’s advice is for people with migraine to open up to a few people who they trust, and educate them about what migraine is, and how it is to live with migraine.
“It really is a battle day-by-day, but that’s why it’s really important to engage with your provider, number one, but also, let a few people in,” says Dr. Lay. “Let them know what’s going on, let them understand how burdensome this migraine is. It’s not simply a headache.”
Conclusion
Key Takeaways for Patients & Caregivers
Chronic migraine is a complex neurological condition that can deeply impact daily life, mental health, and physical well-being.
Patients and caregivers should understand both the physical and emotional aspects of living with migraine, as well as the importance of a comprehensive treatment plan.
While each person’s experience is unique, early diagnosis, personalized treatment, and lifestyle adjustments can greatly improve quality of life.
By building a strong support system and keeping track of symptoms and triggers, patients and caregivers can work together to better manage the condition.
For those living with migraine and their caregivers knowledge is power. Understanding the essentials of migraine management can make a meaningful difference in daily life.
The Importance of Early Diagnosis & Comprehensive Care
Detecting migraine early and receiving thorough care can greatly improve outcomes for those affected. An early diagnosis helps individuals understand their condition sooner, allowing them to manage symptoms before they worsen or become chronic.
Working closely with healthcare providers ensures that each aspect of migraine management is considered, leading to a better quality of life and potentially reducing the frequency and intensity of attacks.
The Outlook for People With Chronic Migraine
One thing that is important for people living with migraine to know, is that chronic migraine is reversible. Around 26% of people who develop chronic migraine go into remission within two years of their condition becoming chronic.7
“The one thing we really don’t want people who are suffering from chronic migraine to do, is to lose hope. Because there’s always hope. It’s a really exciting time in terms of science. We’re understanding more, we’re making newer, different, targeted medications. We also understand more about the importance of things like mindfulness and meditation, and understand now that meditation is critically important,” Dr. Lay says.
There is even hope for those who have felt stuck in chronic migraine for years.
Dr. Lay adds, “We do think that the longer you’re stuck in chronic migraine, the harder it is to get out of it. We know that certain things are good for you to do when you have migraine, but when you have chronic migraine and you’ve got a disabling attack 20, 25, 30 days a month, it’s really hard to follow those lifestyle changes. So, I do think the longer you’re in it, the harder it is to break the cycle, but it doesn’t mean we can’t break the cycle.”
Sinuses have been documented, studied, and pondered since at least the ancient Egyptians’ time. They have a vast array of purposes and benefits for our well-being, including prepping air for inhalation, protecting our brains and immune systems, and shaping our voices. While this structure is incredible and complex, it has limitations. This article explores sinus headaches, their causes, symptoms, and treatment/management options.
Sinuses have been documented, studied, and pondered since at least the ancient Egyptians’ time. They have a vast array of purposes and benefits for our well-being, including prepping air for inhalation, protecting our brains and immune systems, and shaping our voices. While this structure is incredible and complex, it has limitations. This article explores sinus headaches, their causes, symptoms, and treatment/management options.
What is a Sinus Headache?
Definition and Key Features of Sinus Headache
Generally, sinus headaches are caused by inflammation or congestion in the sinuses (i.e., air-filled spaces around the nose, eyes, and forehead). This can occur during a sinus infection (e.g., sinusitis) or severe allergies. Key symptoms include pain and pressure in the face or forehead (often worse with movement), nasal congestion, and sometimes a runny nose or reduced sense of smell.
However, it’s important to note many headaches people think are sinus-related are actually migraine or tension headaches. These types of headaches can mimic sinus pain but aren’t caused by sinus inflammation. In fact, “sinus headache” isn’t an official medical diagnosis. Sinus headaches due to sinus inflammation are relatively rare and usually appear with signs of infection, such as fever, thick nasal discharge, or facial tenderness.1
Common Misconceptions About Sinus Headache
Numerous common myths exist about sinus headaches. Whether from symptom overlap, incorrect patient observations, or even public perception and advertising, these misconceptions can negatively impact identifying, diagnosing and, more importantly, treating and managing sinus headache symptoms.
Myth
Reality
Facial Pain = Sinusitis
Facial pain can also be caused by other headache types (e.g., migraine or tension headache) and have similar symptoms like nasal congestion and pressure.
Sinus Head Pain = Infection
Sinus head pain can be triggered by allergies, air pressure changes, or structural issues (e.g., a deviated septum).
Antibiotics Cure Sinus Headache
Most sinus headaches result from viral infections or noninfectious causes. Antibiotics are only used for the less common bacterial sinusitis.2
Sinus Headache = Migraine
Though some similarities exist (e.g., nasal congestion and facial pain), unlike sinus headaches, migraine headache attacks have distinct symptoms (e.g., nausea, light sensitivity, and throbbing pain).
Weather Change = Sinus Headache
While air pressure and humidity can influence sinus headaches, weather changes can trigger other things as well (e.g., migraine attacks).
Decongestants Always Work
Decongestants can help reduce nasal congestion but may not tackle underlying causes of sinus headaches (e.g., inflammation, infections, etc.).
Sinus Headache = Serious Medical Issue
Many sinus headaches are mild and can be resolved with hydration, rest, and over-the-counter treatments. However, persistent or severe symptoms warrant medical evaluation.
What Causes Sinus Headache?
It can be tricky to determine the root cause of head pain around the sinuses. This was illustrated during the 2021 Migraine World Summit, with Dr. Peter Goadsby discussing the specific nerve pathways that supply pain sensation to the head and face, the ways they impact how and where pain is perceived, and the resulting complex journey to determining cause and treatment.3
However, for sinus-centered headaches, originating from the sinuses, there are some common culprits.
Sinus Infections and Rhinosinusitis Explained
Both sinus infections and rhinosinusitis refer to swelling or inflammation of the sinuses. Although these terms are often used interchangeably, rhinosinusitis is the correct medical term for inflammation of both the nasal passages (rhinitis) and sinuses (sinusitis).4
To recap, sinuses are air-filled cavities located in the skull around the nose, eyes, and forehead, and they produce mucus to trap dust and pathogens. Therefore, sinusitis (aka a sinus infection) happens when sinuses become inflamed, swollen, or infected. There are varying types of sinus infections (i.e., a spectrum of acute to chronic, and allergic vs. non-allergic).
As mentioned above, rhinosinusitis is broader and describes combined inflammation of the nasal passages and sinuses. Causes, symptoms, and classifications are the same as those for sinus infections but focus on both areas. Regardless, both stem from instigators like viruses, bacteria, fungi, allergies/allergens, or anatomy. Read on for more on these last two causes.
Allergens & Environmental Triggers
Since sinus head pain is often linked to inflammation or congestion in the sinuses, allergies and/or environmental factors can trigger or exacerbate these headaches.
Allergies (e.g., allergic rhinitis, more commonly known as hay fever) can cause inflammation in nasal passages and sinuses, leading to a flood of symptoms and resulting in sinus pain. Breaking this down step by step, here is what happens:
An allergen (e.g., pollen, dust, pet dander, mold, etc.) triggers the body to create and release histamines.
Histamine effects are what we notice/experience as inflamed, swollen, and mucus-filled nasal passages and sinuses.
Swelling blocks drainage and traps mucus in the sinuses, and causes pressure/pain (i.e., sinus headache).
Continued exposure to allergens leads to persistent allergies and sinus headaches.
Environmental conditions, on the other hand, can exacerbate sinus inflammation or congestion, contributing to sinus pain. These elements include air quality, weather changes, extreme temperatures, and problematic workplace conditions (e.g., exposure to dust, fumes, or chemicals).
Structural Issues
There are instances where external influences do not cause sinus headaches, nor does the bodily reaction to said factors cause them. Sometimes, our body composition (e.g., anatomical abnormalities blocking normal airflow and drainage) can be the reason for sinus discomfort.4
Deviated Septum and Nasal Polyps
A deviated septum occurs when the nasal wall (the membrane separating our nostrils) is displaced to one side, partly or entirely blocking a nasal passage. As has been said before, blocked sinuses impact drainage, often creating pressure and, as a result, pain that mimics or contributes to sinus headaches.
Nasal polyps are growths (non-cancerous) that develop in the lining of nasal passages or sinuses, often due to chronic inflammation (e.g., from allergies or asthma). Like deviated septums, polyps cut off the flow, resulting in pressure, buildup, and sinus pain.
Symptoms of Sinus Headache
It is worth repeating that these elusive headache types are typically caused by inflammation or blockage in the sinuses, which leads to pressure and pain. Before diving into symptom specifics, exploring how a sinus headache differs from similar headache types is valuable.
Distinguishing Sinus Headache From Other Headache Types
Sinus headaches, migraine, and tension headaches can have overlapping symptoms, making it easy to confuse the three. However, they differ in causes, triggers, and accompanying symptoms.
During the 2023 Migraine World Summit, Dr. Mark Mehle explains just how often sinus headaches can be mistaken for other types of headaches. He also offers advice on determining the cause. Dr. Mehle says, “The timing, and the secondary symptoms are exactly what you want to hang your hat on.” After all, the similarities are so striking. He reiterates, “I think the pain is identical. It really is. It’s just stimulation of the trigeminal nerve — whether it’s stimulated in the sinuses by pus and infection or stimulated centrally by the brain-triggering pain along the trigeminal nerve, is kind of irrelevant. It feels the same to the patient. So, it’s very hard to sort out. And I think that the timing is the key factor, plus those secondary effects.”5
Here’s a brief comparison to help distinguish the differences among these similar headache scenarios1:
Facial pain is a prominent symptom of sinus headaches, which, as stated before, are often caused by inflammation or pressure in the sinus cavities and are directly linked to various factors. Your physician may ask the following questions to help determine a diagnosis.
Where is the pain (i.e., eyes, forehead, and/or cheeks)?
What is the pain like (e.g., sensation type, facial pressure/fullness, and side of the sinuses)?
What triggers the pain (e.g., time of day, movement, or weather)?
What other symptoms are there?
Why is the pain happening (i.e., sinus infection, allergies, and structural issues mentioned earlier)?8
Nasal Symptoms
Another telltale sign of sinus headache is nasal symptoms, which are again due to blockage of the paranasal sinuses. These accompanying symptoms to head pain are often hard to ignore.
This is the feeling of a blocked or stuffy nose due to nasal/sinus swelling, making breathing through the nose difficult. This results in mouth breathing.Thick, often pale mucus (yellow or green) comes from the nose or throat. With nasal discharge, there is a constant need to blow the nose or wipe away mucus. With post nasal drip, there is ongoing throat clearing, coughing, or a scratchy or sore throat.Sinus pressure/congestion brings feelings of pressure, fullness, or tenderness in the face, which typically get worse when moving around or upon first waking up for the day.
At the 2022 Migraine World Summit, Dr. Christopher Gottschalk emphasizes the extent to which the complexities of pain and associated symptoms in such a confined space causes confusion for the individual, as well as for healthcare professionals. For example, he states, “The fact that you’re talking about somebody who gets pain on one side with a red eye and a runny nose and stuffiness, and sometimes fullness in their ear, etc., it is as likely as not to be thought of as some kind of sinus problem. We know that getting diagnosed with sinus headache in migraine is common, and as far as we can tell, there really is no such thing as sinus headache. But in cluster even more so, because there are such clear features of something to do with the sinuses.”7
When to Worry: Risk Factors for Serious Sinus Headache
Symptoms associated with sinus head pain are often benign, but in some cases, they may signal more serious conditions. Red flags, as explained in the table below, are important to pay attention to with sinus headaches, as in some rare cases, they can be signs of:
Serious infections
Vision issues
Structural problems
A weakened immune system
Spreading to other areas
Underlying health difficulties
Sudden emergencies
Timely medical help is vital to prevent long-term damage, avoid life-threatening situations, and ensure effective treatment. Here is a general breakdown of risk factors and warning signs for sinus headaches.2
Risk
Signs
Ongoing/worsening symptoms
Symptoms lasting several days without improvement
Initial improvement followed by worsening symptoms
Facial pain that does not respond to traditional treatments
High fever
Along with chills or severe tiredness
Neural issues
Confusion, disorientation, and low energy
Trouble seeing clearly
Eye problems
Swollen, red, and painful eyes
Trouble moving the eyes
Trouble seeing clearly
Structure abnormalities
History of sinus obstructions (e.g., deviated septum, polyps)
Recent facial injuries/surgeries
Immune system issues
A weakened immune system due to certain conditions of long-term use of specific medications
Frequent sinus infections
Can be due to underlying allergy issues or health conditions
Recent medical history
Dental work/infections or travel to specific regions of the world
Other red flags
Sudden, severe headache
A stiff neck
Swollen/red forehead or cheeks
Trouble breathing
Any of the symptoms above are sufficient reasons to seek professional help. If sinus headaches are frequent or affecting your quality of life, schedule a visit with your doctor to discuss what’s going on and what to do about it.
Sinus Headache Diagnostics & Treatment
History, Examination, & Diagnostic Tools
Diagnosing the cause of a sinus headache, like other ailments, begins with a medical history and physical exam. Doctors will ask about symptoms, including duration, triggers, and associated factors. During an exam doctors may check for facial tenderness, examine nasal passages using specific tools, and assess for other conditions (e.g., migraine headaches and tension headaches) that mimic sinus headaches’ symptoms.11
If the above assessment strategies are inconclusive, other diagnostic tools are sometimes used, including:
X-rays
CT scans
Allergy tests
Nasal endoscopy (a tube with a camera that goes into the nasal passages)
As mentioned earlier, since other types of headaches originate in a similar area as headaches caused by sinusitis, individuals, including health professionals, can find it challenging to know what is happening. Hence, further tests may be warranted.
Once it’s confirmed that a person has a sinus headache, the next step is to find the appropriate treatment to relieve symptoms and address underlying causes.10
Home Remedies and Natural Solutions
Treatment
How It Works
Steam inhalation
Loosens mucus and reduces congestion
Humidifier
Adds moisture to the air, draining sinuses
Warm compress
Eases sinus pressure and improves blood circulation
Hydration
Thins mucus and eases drainage from sinuses
Essential oils
Have anti-inflammatory and decongestant traits
Nasal irrigation
Flushes out allergens, irritants, and mucus from nasal passages
Over-the-Counter (OTC) Medications for Sinus Relief
There are three main OTC medications for sinus headaches available without a prescription. They are:
Antihistamines
For sinus headaches triggered by allergies
Reduce inflammation and mucus production
Decongestants
Available as sprays or tablets
Relieve nasal congestion and reduce sinus pressure
Nasal corticosteroids
Minimize inflammation and improve sinus drainage
Prescription Medications for Sinus Relief
Antibiotics and higher-potency decongestants require a medical professional’s visit and prescription. Antibiotics are only used to treat bacterial sinus infections, not viral or allergy-related sinus issues. Strong decongestants can also tackle severe or chronic cases of inflamed sinuses.11
Prevention
Preventing sinus headaches requires a proactive and holistic approach. By managing allergies, maintaining healthy sinuses, and making key lifestyle adjustments, the frequency and severity of sinus headaches can be reduced.12
Managing Allergies and Avoiding Triggers
Since allergies are a common cause of sinus inflammation and head pain, identifying and avoiding allergens can play a huge role in prevention. This can include identifying and, if possible, avoiding culprit allergens (e.g., pollen, dust, or dander). Using things like air purifiers, washing your bedding often, and vacuuming regularly can also minimize allergens in your frequently occupied spaces.
Keeping Your Sinuses Healthy
Healthy sinuses involve keeping nasal passages clear and reducing irritants contributing to inflammation. Small and consistent habits can make a big difference, including:
Long-term relief from sinus headaches often requires changes to daily habits. Adjustments to your routine can prevent future episodes and improve your overall quality of life. Managing stress through relaxation techniques (e.g., yoga, meditation, or deep breathing) can reduce inflammation and support immune function, lowering the risk of sinus infections. Regular exercise improves circulation, which helps clear nasal passages and boost immunity. Avoiding sudden or significant temperature changes prevents nasal passage constriction, reducing mucus buildup and the likelihood of congestion-related headaches.10
Living With Chronic Sinus Headache
Chronic sinus headaches can significantly impact day-to-day life, but there are approaches and resources to help manage symptoms. For example, managing chronic sinus disease involves recognizing symptoms early and reducing stress to minimize flare-ups. Consistent self care can make a big difference.
It is also important to mention that living with ongoing sinus headaches can leave people feeling very alone, but that need not be the case. Support groups and reliable resources can provide valuable information and emotional support. One option is to join support groups (local or online) to connect with others dealing with chronic sinus headaches or refer to trusted resources (e.g., medical organizations or clinics) for up-to-date treatment options and advice.8
Conclusion
Sinus headaches can be complicated, but understanding their causes and treatments can empower you to manage them well. Prevention, early diagnosis, and timely treatment are key. If symptoms continue or worsen, seek the right help to find the solutions right for you, and get control over your health again.
Patel, Z. M., Setzen, M., & Poetker, D. M. (2009). Sinus headache: Avoiding over- and mis-diagnosis. American Journal of Rhinology & Allergy, 23(4), 325–329. Retrieved from https://pubmed.ncbi.nlm.nih.gov/19344297/
Schreiber, C. P., Hutchinson, S., & Dodick, D. W. (2005). Sinus headache: A neurology, otolaryngology, allergy perspective. Cephalalgia, 25(1), 43–49. Retrieved from https://pubmed.ncbi.nlm.nih.gov/16007896/
Supports
National Headache Foundation: This organization offers educational materials, patient assistance programs, and community support for those experiencing various headache disorders, including sinus headaches. Its website provides access to resources such as patient stories, podcasts, and tools for managing headache symptoms.
American Migraine Foundation: This foundation offers resources to help people connect with others who understand the challenges of living with headaches, including sinus-related headaches.
Miles for Migraine – Migraine Support and Community Groups: Brings together individuals to connect, share, and discover resources related to migraine and headache disorders. These groups offer supportive discussions and helpful materials to better navigate life with head pain, including sinus headaches.
Mayo Clinic Connect: Online community where patients can share experiences and find support related to sinus infections and associated headaches, offering a platform to connect with others facing similar health issues.
Asthma and Allergy Foundation of America (AAFA): Provides support for individuals with asthma and allergies, which can be related to sinus issues. It offers online communities and local support groups for patients seeking assistance and connection.
A silent migraine, also known as an acephalgic migraine, is a type of migraine that presents with the typical aura phase of a classic migraine but doesn’t include head pain. Silent migraine is also referred to as aura without headache.13 A silent migraine may also include the prodrome and postdrome symptoms of a common migraine but without the head pain, most commonly associated with a migraine attack. Silent migraine occurs in 5% of the migraine population and the diagnosis is more common in people after the age of 50.
A silent migraine, also known as an acephalgic migraine, is a type of migraine that presents with the typical aura phase of a classic migraine but doesn’t include head pain. Silent migraine is also referred to as aura without headache.13 A silent migraine may also include the prodrome and postdrome symptoms of a common migraine but without the head pain, most commonly associated with a migraine attack. Silent migraine occurs in 5% of the migraine population and the diagnosis is more common in people after the age of 50.1,2
In a 2023 interview with neurologist Dr. Nazia Karsan, a postdoctoral clinical fellow of King’s College in London, Lisa Horwitz of the Migraine World Summit illustrates how debilitating migraine symptoms, beyond head pain, can be.11
I find that the accompanying symptoms can be even more disabling than the pain. A person can get used to the pain, but it’s hard when you’re not cognitively at your best, and you still have to work, or parent, or drive a car.
Symptoms of Silent Migraine
A range of disabling symptoms are possible, affecting various senses. Several of the most common symptoms of silent migraine attacks are explained below.8
Visual disturbances: Also known as scintillating scotoma, includes flashing lights, zigzag patterns, or blind spots.
Sensory changes: Tingling, numbness, and hot or cold sensations — especially in the face, hands, and feet.
Speech difficulties: Also known as aphasia, includes trouble finding words or speaking clearly.
Dizziness, vertigo, or tinnitus: A sensation of spinning, losing balance, or ringing in the ears.
Nausea and vomiting: Feelings of sickness without any apparent cause.
Photophobia and phonophobia: Sensitivity to light and sound.
Irritability: feeling grumpier than usual, easily aggravated.
Fatigue: experiencing extreme tiredness.
Phases of Silent Migraine
Silent migraine may or may not present with phases.
Like a migraine attack with head pain, a silent migraine may be preceded by symptoms known as the prodrome phase. This phase can start anywhere from a few hours to a few days before a person experiences a silent migraine attack or aura.
1) Migraine Prodrome
The migraine prodrome may express with any or several of the following symptoms, up to 24 hours before an aura:
Irritability
Depression
Fatigue
Excessive yawning
Urinating more than usual
Trouble sleeping
Food cravings
Nausea
Increased sensitivity to light or sound
Difficulty concentrating, reading, or speaking
Neck pain or stiffness
Hyperactivity
2) Migraine Aura
This is the second phase of a migraine for those who experience migraine with aura. Migraine aura can induce various changes throughout the body, including: visual aura (such as flashing lights or zig zags), sensorimotor aura (such as tingling, numbness, or weakness), and dysphasic aura (such as mumbling or slurred speech).
A person diagnosed with vestibular migraine may have aura symptoms of dizziness or vertigo. If they experience these symptoms without the accompanying head pain, it is considered a silent migraine.10 For a person diagnosed with abdominal migraine, a silent migraine may include loss of appetite, nausea, or vomiting, but no head pain.
A person diagnosed with visual aura and silent migraine may see wavy lines, bright lights, flashing dots, or sparkles. These may seem to start in the center of a person’s line of sight and spread to both sides of their field of vision. Silent migraine with visual aura may also include blind spots or scotomas, but with no accompanied head pain.
No, a defining characteristic of silent migraine is a lack of the throbbing head pain that is a hallmark of a typical migraine attack.
4) Migraine Postdrome
The last phase of silent migraine is the postdrome phase. Not everyone with silent migraine will experience a postdrome. For those who do, the postdrome phase can include feelings of euphoria for some people. For others, feelings of depression can occur, or symptoms similar to those experienced during a hangover from excess alcohol consumption. A postdrome can last anywhere from a few hours to a few days.
Postdrome symptoms may include:
Fatigue
Body aches and sore muscles, such as a stiff neck
Difficulty concentrating or brain fog
Nausea
Light sensitivity
Sound sensitivity
Dizziness
Mood changes, ranging from euphoria (extreme happiness) to depression
Did you know?
Did you know a silent migraine can last anywhere from a few minutes up to several hours?13
Silent Migraine Triggers?
Silent migraine shares many of the same triggers as common or classic migraine, such as:3
Foods and drinks including alcohol, chocolate, and nuts, as well as those foods containing the amino acid tyramine (found in red wine and aged cheese), artificial sweeteners like aspartame, artificial coloring, and additives.
Environmental factors such as bright or flickering lights, and sudden or loud noises.
Physiological changes such as hormones during menstruation, pregnancy, or menopause; low blood sugar; and dehydration.
Stress due to sensory and emotional overload, or physical exhaustion.
Headache experts say keeping a daily diary is an important step in diagnosis and in understanding silent migraine triggers. By tracking what a person eats and drinks, changes to their sleep, as well as their hormones, stress levels, and other possible triggers, a diary makes it easier to properly diagnose silent migraine and prevent future migraine attacks. Silent migraine attacks and visual aura are highly correlated, and research is continuing to improve our understanding of this correlation.6
Silent Migraine Causes
Similar to what causes common migraine, migraine aura without headache develops due to a combination of genetic, environmental and lifestyle factors, some of which remain unknown. Variations in many genes have been found to be associated with the development of migraine with and without aura, and migraine tends to run in families. Most of the associated genes are active in the vascular smooth muscle in the brain.
Cortical Spreading Depression (CSD) is linked to aura with migraine.1 It is believed that CSD is also a factor in silent migraine. CSD happens when brain cells in the cerebral cortex become hyperactive and then become inactive in a wave that spreads across the cortex. This decrease spreads across the top layer, or cortex, of the brain. It often travels from the visual part of the brain (occipital lobe) to the body sensation part of the brain (parietal lobe) to the hearing part of the brain (temporal lobe) and is linked to blood flow and changes in serotonin levels.3
The cerebral cortex is the outermost layer of the brain’s nerve cell tissue, also referred to as gray matter. Researchers believe genetic mutations may cause CSD that leads to migraine aura. Some of the factors that may contribute to CSD include:
emotional stress
hormonal fluctuations
changes to sleep (including oversleeping or not getting enough sleep)
weather changes
exposure to bright lights, loud sounds, or strong odors
skipping meals
In an interview with the Migraine World Summit, Carl Cinncinato asks neurologist, ophthalmologist, and board-certified headache specialist Dr. Kathleen Digre: “Is it the electricity that’s the change that’s causing the cortical spreading depression or is it a lack of blood flow or something else?”
Dr. Digre says: “What’s interesting is that it is sort of an electrical slowing instead of a seizure. If somebody has a seizure or epilepsy, they have firing of their neurons causing the seizure, but this is something different. Things slow down. There’s this slow wave that goes across the brain, and there are vascular changes that do occur in … There’s some fascinating videos that show this coupling of the slow wave with the vascular changes that are present in the brain, and I think it’s something that’s been demonstrated, for example, in the cortex of other animals.”
Who Gets Silent Migraine?
Silent migraine, or aura without headache, is a subset of migraine. It occurs in 4-5% of patients with migraine regardless of gender. For people who have migraine with aura it may occur at some point in 38% of patients. Typical aura without head pain commonly presents as visual aura. It may also present as a brainstem aura without head pain, presenting as slurred speech, ringing in the ears, impaired hearing, uncoordinated movements, and vertigo. When silent migraine develops later in life, it is classified as late-onset migraine.4
Did you know?
Did you know migraine, including silent migraine, is more common in women? This is believed to be due to female hormones, the menstrual cycle, pregnancy, and menopause.16
Diagnosing Silent Migraine
Silent migraine can present similar to other conditions because it lacks the head pain that goes along with a classic or common migraine. For example a person with migraine who has been diagnosed with brainstem aura may experience the following symptoms:9
Dysarthria (slurred speech)
Vertigo (feeling of movement/spinning of self or environment)
Tinnitus (ringing in ears)
Hypacusis (impaired hearing)
Diplopia (double vision)
Ataxia (unsteady/uncoordinated movements)
Decreased level of consciousness
In rare cases, a person’s symptoms may be a sign of a different or more serious medical problem, such as a stroke or bleeding in the brain. In order to rule out other, more serious or life threatening, medical conditions, healthcare providers diagnose silent migraine by doing a physical examination and may perform neurological testing, such as CT or MRI scans.
During the 2023 Migraine World Summit Dr. Karsan shared that the onset of symptoms is often what may provide the biggest clue.11
She says, “I think the onset is very important. So, if it’s like a very sudden one minute I’m fine, the next minute I have a symptom, that’s always of concern. I think the evolution of those symptoms is really important. So, do they just come and then stay fixed, or do they sort of move around and spread?”
She further explains, “Aura is much more likely to have this sort of spreading phenomenon where, for example, tingling can start in one area and then spread up the arm and down the leg, for example, over some minutes. That’s less likely to happen with a stroke than it is with aura. But I would say generally my rule is if you have something that’s new and focal that you’ve not had before, you should seek attention.”
And Dr. Karsan has special advice for older people. “If you have something that you think is aura, but you’ve never had an aura before, and you are over 50, that’s something that should seek attention.”
Comorbidities of Silent Migraine
Several neurological and psychiatric disorders often coincide with silent migraine5. These comorbidities include:
Depression and anxiety
Mood disorders
Epilepsy
Neuronal hyperexcitability
Sleep disorders
Treating Silent Migraine
Silent Migraine and Thresholds
Because migraine is considered a threshold disease or disorder, the frequency, duration and intensity of migraine attacks can sometimes be moved up or down by various factors3. These include triggers and lifestyle choices.7 In an interview with the Migraine World Summit in 2021, Dr. Sait Ashina, assistant professor of neurology and anesthesia, discusses migraine as a threshold disease.15
Helpful Lifestyle Choices
The following behaviors and lifestyle choices are helpful in the prevention of migraine — and also good for overall brain health and longevity.
Eat regular, healthy meals. Enjoy foods with a lower glycemic index.
Stay hydrated.
Limit alcohol.
Be consistent with your caffeine intake.
Avoid processed foods, additives, and coloring agents.
Perform regular low-impact exercise.
Get adequate, consistent sleep.
Take part in meditative, mindful, and relaxing practices.
Manage stress.
Sometimes, however, migraine can worsen despite all reasonable attempts to improve lifestyle choices. After all, some migraine triggers are unavoidable, such as hormonal fluctuations, unexpected stressful events, and the weather.
Medication for silent migraine is centered on the prevention of attacks and easing of symptoms. According to the International Headache Society’s newly released Global Practice Recommendations for Preventive Pharmacological Treatment of Migraine, preventive medicine is recommended for individuals when one or more of the following conditions are met.14
The person has four or more attacks per month.
Their migraine attacks have had an impact on their personal, social, or professional life.
Their acute treatment proves ineffective.
Their acute treatment has to be taken too often.
Preventive medications include:
Blood pressure-lowering drugs, including beta-blockers like metoprolol (Lopressor) and propranolol (Inderal), and calcium channel blockers, such as verapamil (Verelan)
Tricyclic antidepressants like amitriptyline and nortriptyline
Calcitonin gene-related peptides (CGRP) monoclonal antibodies such as eptinezumab-jjmr (Vyepti), erenumab-aooe (Aimovig), fremanezumab-vfrm (Ajovy), and galcanezumab-gnlm (Emgality)
Gepants like atogepant (Qulipta) and rimegepant (Nurtec ODT)
Anti-seizure drugs like topiramate (Topamax) and valproate
OnabotulinumtoxinA (Botox) shots
Medications that treat acute migraine attacks, include:
Acetaminophen (Tylenol)
NSAIDs such as Ibuprofen or Aspirin
Anti-nausea medicines (antiemetics) like ondansetron (Zofran)
Triptans such as eletriptan (Relpax) and sumatriptan (Imitrex)
Gepants like rimegepant (Nurtec ODT), ubrogepant (Ubrelvy), and zavegepant nasal spray (Zavzpret)
Finding the right combination of medications for optimum silent migraine treatment, as well as prodrome and postdrome symptoms, may take some trial and error according to Dr. Karsan. She says, “I think incorporating those bothersome symptoms outside of headache, and perhaps outside of what we recognize as canonical migraine symptoms, will really take us forward in understanding how these drugs may work in that process.”
Silent Migraine Best Practices
Track your migraine attacks with a headache diary, calendar, or app to better understand your triggers and how migraine affects you.
Develop a migraine management plan in consultation with your doctor that is appropriate for the frequency and severity of your attacks. The plan may include acute treatment, preventive therapies, and lifestyle changes.
If your condition does not improve or the burden of symptoms is high, consider consulting with a headache specialist via a referral for a more robust and comprehensive management plan.
Remember that making changes to your lifestyle for migraine is also good for your overall brain health and longevity. None of us lead a perfect lifestyle, but to the extent we can make improvements, however small, to better manage stress, improve sleep, become more physically active, and make healthier food choices, the better for our overall health and well-being.
Takeaways
Silent migraine, or aura without headache, is a condition that causes aura symptoms, such as vision changes, sensorimotor changes, language changes and more, without the head pain of a typical migraine. The same factors that can trigger a classic migraine headache can also trigger a silent migraine, including weather changes, hormonal changes, stress, certain foods, dehydration, bright lights, and loud noises.
Managing silent migraine starts by understanding how migraine affects you, and developing an appropriate management plan in partnership with your doctor. Both lifestyle modifications and medication can help prevent and treat this condition.
Silent Migraine FAQs
What is a silent migraine like?
A silent migraine involves sensory symptoms such as flashing lights, dizziness, tingling, numbness, nausea, vomiting or speech difficulties without a headache.
Can dehydration cause a silent migraine?
The same triggers that can contribute to common and classic migraine can contribute to silent migraine. Dehydration is a known migraine trigger, which is why it’s important to stay hydrated by drinking plenty of fluids.
What is the difference between vestibular migraine, abdominal migraine, and silent migraine?
Vestibular migraine is a type of migraine that causes dizziness, and it may or may not include a headache. Abdominal migraine is a type of migraine that causes appetite loss, nausea and/or vomiting; it may or may not present with head pain. Silent migraine does not include a headache.
What is the difference between silent migraine and complex migraine?
Complex migraine is not an official migraine type; it means different things to different headache specialists. Typically, those specialists who are trained specifically in migraine do not use the term “complex” as they are able to correctly diagnose migraine subtypes.
Are aura symptoms without migraine dangerous?
A silent migraine, or aura symptoms without the head pain of a migraine attack, can feel scary, especially if a person is having one for the first time and has not yet received a diagnosis. However, a silent migraine is not life-threatening or more serious than a common migraine or classic aura.
What is migraine without aura?
Migraine without aura is a moderate to severe throbbing headache that comes on without a visual aura (changes to vision such as flashing lights, zigzags, blind spots) preceding it. It’s the most common type of migraine.
Calcitonin gene-related peptide (CGRP) inhibitors represent a new class of drugs uniquely designed to treat migraine. There are two types of CGRP inhibitors: monoclonal antibodies which are designed for migraine prevention, and gepants which can be used as both preventive and acute migraine therapies. Several options are available within both categories. While these treatments are not a cure for migraine disease, they have proven to be safe and effective.
Calcitonin gene-related peptide (CGRP) inhibitors represent a new class of drugs uniquely designed to treat migraine. There are two types of CGRP inhibitors: monoclonal antibodies which are designed for migraine prevention, and gepants which can be used as both preventive and acute migraine therapies. Several options are available within both categories. While these treatments are not a cure for migraine disease, they have proven to be safe and effective.
What is CGRP?
CGRP is the acronym for calcitonin gene-related peptide. CGRP is a small molecule made up of 37 amino acids that is produced naturally by the body.1 CGRP is involved in body functions in the gut, the reproductive tract, and blood vessels.2
CGRP may be helpful in protecting against cardiovascular issues, such as high blood pressure and heart disease. For example, in the midst of a heart attack or a stroke, CGRP may be released to help prevent such an event.1
While CGRP is found in everyone and is helpful to some of our body functions, the effects of CGRP can also contribute to migraine attacks.
What is the role of CGRP in migraine?
CGRP is released into the body during the migraine process.18 CGRP affects the trigeminal nerve, which communicates pain and sensitivity to touch and temperature. It is released throughout the peripheral and central nervous systems during a migraine attack. When CGRP attaches to its receptors in the brain, it perpetuates the migraine process, leading to inflammation and headache pain.3 4In patients who have chronic migraine disease, CGRP levels remain elevated during a migraine attack, as well as between attacks.19
Did You Know?
The trigeminal nerveis the largest of the 12 cranial nerves that connect the brain to the body. Specifically, the trigeminal nerve connects to sensory and motor functions in 3 areas:
upper part of the face, including the forehead, scalp, and upper eyelids
middle part of the face, including the cheeks, upper lip, and nasal cavity
lower part of the face, including the ears, lower lip, and chin, controlling the movement of muscles in the jaw and ear.20
Clinical studies have shown that when CGRP is injected into the body it causes moderate to severe headaches in people who have not been diagnosed with migraine disease, and migraine-like headaches in people who have migraine disease.1 18 This information suggests that people with migraine disease may be particularly sensitive to CGRP.18
The initial development and studies of drugs that target and reduce the amount of CGRP in the body began in the late 1990s.18 The first CGRP inhibitors to prevent, reduce, and or treat migraine attacks were approved by the FDA in 2018.3
Did You Know?
Migraine medications that block CGRP may also be known as:anti-CGRP medications
CGRP inhibitors
CGRP receptor antagonists
CGRP monoclonal antibodies for migraine
gepants
What are CGRP Inhibitors?
CGRP inhibitors generally fall into two classes of drugs: Monoclonal antibodies and receptor antagonists.3
Monoclonal antibodies
Monoclonal antibodies work by blocking the CGRP pathway. They are a preventive treatment due to the longer duration they remain in the bloodstream.1Monoclonal antibodies are FDA approved for migraine with and without aura.6
The following monoclonal antibodies work by binding to the CGRP molecule itself, “mopping up” the CGRP in the body.7 They are FDA approved for the preventive treatment of migraine in adults.
Fremanezumab (Ajovy) is self-administered as a subcutaneous injection every month or every 3 months, depending on dosage.8
Galcanezumab (Emgality) is self-administered as a subcutaneous injection every month for the preventive treatment of migraine. A different dosage is approved for the treatment of episodic cluster headache.9
Eptinezumab (Vyepti) is administered in the doctor’s office as a 30 minute intravenous infusion every 3 months. It is approved for the preventive treatment of migraine in adults.10
A fourth FDA approved option, erenumab (Aimovig), works by binding to the CGRP receptor, so that the CGRP cannot be activated and result in a migraine attack.7 Aimovig is self-administered as an injection every month, and is approved for the preventive treatment of migraine in adults.11
Gepants
Gepants are small molecule CGRP receptor antagonists that bind to and block CGRP receptors. Gepants are generally marketed for acute migraine treatment due to the shorter length of time they stay in the bloodstream, but some gepants may be used daily as a preventive treatment.1 4 5 12 13
The following gepants are FDA approved for the acute treatment of migraine in adults:
Rimegepant (Nurtec ODT) is a disintegrating 75 mg single dose oral tablet. It is also approved for the preventive treatment of episodic migraine.14
Ubrogepant (Ubrelvy) is prescribed as a 50 or 100 mg oral tablet. A second tablet can be taken in 2 hours if the migraine pain returns. The maximum dose is 200 mg per day.13 It is approved for the acute treatment of migraine attacks with or without aura; it is not approved for the prevention of migraine headaches.15
A third option, atogepant (Qulipta) is FDA approved for the preventive treatment of episodic migraine in adults. It is prescribed as a daily 10 mg, 30 mg, or 60 mg oral tablet.16 At this time it is not FDA approved for acute migraine treatment.
Did You Know?
A key attribute of gepants is that they do not cause rebound headache (medication overuse headache).12 Learn more about rebound headache.
Risks
What are the side effects?
Side effects of the CGRP monoclonal antibodies include:
constipation11
high blood pressure11
injection site reactions, such as pain, redness, or swelling8 9 10 11
Side effects of gepants include:
constipation16
fatigue15 16
nausea14 15 16
Who is contraindicated?
CGRP inhibitors are generally well tolerated and can be used safely by patients who do not have an allergic reaction to the drug or its ingredients.
Before taking the drug, patients should tell their healthcare provider about all medical conditions and medications, as some interactions may exist.
CGRP inhibitors have not been adequately studied for safety in pregnant women, unborn infants, or their presence and effect in human milk, milk production, or breastfeeding infants.13 19 Patients should tell their healthcare provider if they are pregnant, breastfeeding, plan to become pregnant, or plan to breastfeed.
Safety and effectiveness in children has also not been established.19 None of the CGRP inhibitors discussed in this article have been approved for the treatment of migraine in children.
How much relief can be expected?
In clinical trials, more than half of people found that their migraine days and/or severity of their migraine attacks dropped by 50% when using a CGRP inhibitor.4 Fortunately, about 70% of people see some level of improvement.17
Some people may need to take the medication for three to six months to achieve an optimal response.4 6There is currently no method to predict who will have good results, and which drug within the treatment class will be the most effective.2 If a patient does not find relief on one CGRP inhibitor, or has not tolerated it due to side effects, it is advisable to try another drug.12
CGRP inhibitors can be an equally effective option regardless of whether you have:
Failed to see migraine improvement on one or dozens of other preventive therapies.
Been using or overusing acute medications.
Been newly diagnosed with migraine disease or have had migraine for a lifetime.
Costs
With a new class of medication such as CGRP inhibitors, there may be challenges for patients to access these treatments. Commercial insurance companies in the U.S. generally require failure of at least two, if not three, preventive medications from three different classes before providing prior authorization to cover these new medications. This is usually due to the high cost of the CGRP inhibitors.6 Without insurance coverage, a year of treatment with a CGRP inhibitor can cost a patient several thousand dollars.13
To assist patients in obtaining these medications, some drug companies offer programs that offer free trial doses, temporary coverage of medication, or copay assistance. These programs may not be available to patients who have government insurance.4
Summary
CGRP inhibitors are the first medications specifically designed for the prevention and treatment of migraine attacks. They have few side effects, and a high degree of efficacy in reducing migraine frequency and/or severity. While cost and insurance coverage of these new medications may pose a challenge for some patients, there are payment assistance programs available. CGRP inhibitors bring new hope to many patients who have struggled to find an effective migraine treatment.
Additional Resources
Links to outside organizations and articles are provided for informational purposes only and imply no endorsement on behalf of Migraine World Summit.
Triptans are a class of drugs specifically designed for the acute episodic treatment of migraine attacks. The first triptan, sumatriptan (Imitrex), was available for the abortive treatment of migraine in 1992, making triptans a well-established migraine treatment option today. Triptans are often one of the first drugs prescribed to individuals living with migraine. Today, there are seven different types of triptans that have emerged since the early 1990s.13
Triptans are a class of drugs specifically designed for the acute episodic treatment of migraine attacks. The first triptan, sumatriptan (Imitrex), was available for the abortive treatment of migraine in 1992, making triptans a well-established migraine treatment option today. Triptans are often one of the first drugs prescribed to individuals living with migraine. Today, there are seven different types of triptans that have emerged since the early 1990s.13
In an interview with Dr. Messoud Ashina, professor of neurology at the University of Copenhagen in Denmark, Paula Dumas of the Migraine World Summit asks about the 10-step treatment plan for migraine.2
Types of Triptans
Triptans are often where physicians’ playbooks start, as today they remain a first-line acute treatment for migraine. There are seven different types of Triptans: 5,13
Did you know that for a migraine drug to be approved by the American Food and Drug Administration (FDA) it needs to have higher efficacy than a placebo in a double-blind study?
How Triptans Work
Triptans are serotonin reuptake inhibitors, also known as serotonin agonists and vasoconstrictors. This means triptans bind to serotonin receptor sites to both stabilize serotonin levels and inhibit the release of calcitonin gene-related peptide (CGRP). At the same time, triptans cause blood vessels to constrict (vasoconstriction).6 Triptans bind specifically to serotonin sites 5HT1B and 5HT1D, which changes the way pain is communicated by the cranial nerves to the brain.13 Through vasoconstriction, there is less blood flow to the brain, which is believed to reduce pressure placed on the blood vessels. It lessens the inflammatory pain experienced during a migraine attack.4
Dr. Deborah Friedman, neurologist, headache specialist, neuro-ophthalmologist and adjunct professor at Thomas Jefferson University, tells us at the 2022 Migraine World Summit, “In the early ’90s, the triptans came along. And the triptans were specifically designed to treat migraine; they targeted, directly, the serotonin receptors, and they changed people’s lives. So, you know, triptans and some of the ergotamines were the first targeted therapies specifically made for migraine.”2
If one triptan doesn’t work for you, another triptan might.
Each type of triptan has a slightly different effect on the body. For example, the half-life of frovatriptan is 26 hours compared with sumatriptan, which is 1-4 hours. Triptans have a greater than 50% efficacy rate for most people. Some people may respond to one triptan and not another, or find that one triptan works better than another. Deciding which triptan is best for you is determined by a discussion with your doctor. Your health profile, diagnosis, and personal medical history will be taken into account.2,5,13
Triptans can be taken orally, through a nasal spray, or via a subcutaneous injection. Nasal sprays and injections are well-suited for people who may experience nausea and vomiting with migraine attacks, making them unable to absorb oral medication in their system. Nasal spray and injections are also faster-acting, which makes them especially helpful for people who wake up with a migraine.
Triptan Dosage and Administration
Below are the seven triptans available for the acute treatment of migraine.6
Triptan Type
Administration
Possible Side Effects7
almotriptan (e.g., Axert)
oral/tablet
dizziness, drowsiness, nausea, sensations of tingling or warmth
eletriptan (e.g., Relpax)
oral/tablet
dizziness, drowsiness, nausea
naratriptan (e.g., Amerge)
oral/tablet
dizziness, drowsiness, nausea
rizatriptan (e.g., Maxalt, Maxalt Mlt)
oral/tablet
dizziness, drowsiness, nausea, sensations of tingling or warmth
In an interview with Dr. Messoud Ashina in 2022, Paula Dumas of the Migraine World Summit asks: “Is there any reason why everyone shouldn’t use a triptan, [or newer drugs such as a] ditan, or a gepant?”
Dr. Ashina replies,
“How is it possible that after 30 years of having triptans on the market … we still have a quite large number of patients who have never tried triptans, or who have tried only one triptan? And with the introduction of the new medications, such as gepants and ditans, we will be forced to try triptans because of the reimbursement rules. … That’s why the optimization of acute treatment should be something every neurologist and GP remembers.”8
Triptan Efficacy
Published in September, 2024, a systematic review and network meta-analysis compared all licensed drug interventions for the acute treatment of migraine attacks in adults. Overall, eletriptan, rizatriptan, sumatriptan, and zolmitriptan had the best profiles. They also were found to work more effectively than newer drugs including lasmiditan, rimegepant, and ubrogepant.17
See the image below, from bmj.com, for more details on the comparisons.
Triptan Side Effects
Side effects of triptans include the following:18
Chest Pain (rare)
Dizziness
Drowsiness, Fatigue
Flushing
Nausea
Neck Pain
Sweating
Tingling, Numbness or a Pins and Needles Feeling in the Hands and Feet
Weakness
Triptan Safety in Special Populations
People With Heart Conditions
Triptans are contraindicated, not considered safe, for people with heart conditions and vascular disease like high blood pressure, Raynaud’s, heart attack, stroke, etc. Dr. Gretchen Tietjen, professor emerita of neurology at the University of Toledo, provided insight on this in her interview on “Migraine Changes in Older Adults” during the 2023 Migraine World Summit.22
Dr. Tietjen says, “One of the things I think that has always vexed people the most, until hopefully recently, now that we have some new drugs that could replace it, but acute medications like the triptans cause vasoconstriction, which means any blood vessel in your body, which has this type of receptor on it — the serotonin receptor of a certain type — if you had that drug in your system, it could cause some — potentially it could cause some vasoconstriction of your coronary artery disease. Now, that is not common at all, but it’s not unheard of.”22
She adds, “That’s why with those drugs, once a person develops cardiac disease and has had a heart attack or has angina symptoms — which is sort of a warning for a heart attack — it’s thought, ‘do not use that medication anymore.’”22
Senior Citizens
Triptans are regularly prescribed to seniors without major vascular or cardiac concerns; however, more studies are needed on the 65+ population. Two recent studies suggest older adults using triptans for migraine may have low increased stroke risk. Still, the researchers of those studies advise, “Migraine treatment in the older population requires careful consideration of increased medical comorbidities.”
Children and Adolescents
Triptans are prescribed less often in children; ibuprofen is recommended for initial treatment for those under age 12.21 Rizatriptan is the only FDA-approved triptan for use for all children ages 6-17.20
In adolescents, sumatriptan/naproxen tablets, sumatriptan nasal spray, and rizatriptan or almotriptan oral-dissolving tablets are recommended for initial treatment. Abortive medications are more effective when used early after the onset of migraine in adolescents and adults.21
Pregnant Women
During the 2017 Migraine World Summit, Paula Dumas and Dr. Matthew Robbins, associate professor of neurology at Weill Cornell Medical College, New York-Presbyterian Hospital, discussed migraine treatment during pregnancy. In regard to triptans, he says, “The tradition has always been to avoid triptans in pregnancy because of the potential for birth defects or the potential to reduce blood flow through the placenta, but recent large studies and registry studies over a decade or more have not shown a major signal of elevated birth defects when compared to the general population, so there is a trend nowadays of using triptans on occasion in those who already have a track record for responding to them before their pregnancy, as long as it’s done in moderation.”19
Nursing Mothers
Dr. Robbins also shared advice on triptan use during breastfeeding. He says, “The general principle for breastfeeding is looking at the ratio of a medicine in milk to plasma, and every medicine has this known ratio, so those that have these lower ratios are safer than those that have the higher ratios, and it has to do with protein binding and other features.”
He adds, “So, for example, of all the triptan medications, eletriptan, which has the brand name Relpax, is probably the safest, because it’s cleared the least into breast milk. But also other considerations have to be taken into account; so, for example, if a woman is breastfeeding a baby who was born premature, and there are crucial concerns about neurological development of that baby, you might really avoid any medications that might impact alertness or awareness that could have deleterious consequences.”19
When to Use a Triptan
Triptans work best if taken at the first signs of a migraine attack, or within the first two hours of migraine onset. The earliest signs of a migraine attack include prodromal symptoms such as yawning, fatigue, irritability, and food cravings. At the first signs of a migraine attack, it is up to the individual to determine if they will choose a triptan to abort the migraine or use an NSAID, analgesic, or other treatment option.10
Did you know?
Did you know triptans work well with some over-the-counter medications, such as NSAIDS and acetaminophen?1
Combinations/Layering Strategies
Triptans, NSAIDS, and Analgesics
Triptans work well with some non-steroidal anti-inflammatory drugs (NSAIDs).1
Common over-the-counter NSAIDs include naproxen (e.g., Aleve) and ibuprofen (e.g., Advil, Motrin). Some triptans, such as sumatriptan, also come with naproxen added.1 Triptans also work well with acetaminophen (e.g., Tylenol, FeverAll), which is a common analgesic. Some people choose to use an NSAID and/or acetaminophen at the first signs of a migraine attack since:
a) Triptans are not to be used more than 10 times per month. b) Not all migraine attacks may require a triptan.
If the migraine attack recedes, the individual may not need to use a triptan. If the attack does not recede within the first two hours of symptom onset, then a triptan is still available for use.
Triptans and Medication Overuse Headache (MOH)
Triptans should not be used more than 10 times per month. This makes triptans effective for the acute treatment of episodic migraine less than 10 days per month. Episodic migraine is defined as having less than 15 attacks per month.8
When triptans are overused, or overused in conjunction with NSAIDs or acetaminophen, people can develop a complication called medication overuse headache (MOH). MOH can present as a daily dull headache or a daily migraine. In most cases, reducing the use of the offending medication will reverse MOH. In some cases, MOH leads to chronic migraine. Chronic migraine is a condition defined as 15 or more headache days per month, with at least eight of those being migraine attacks, for at least three months.8,11
Often people living with migraine are continually searching for the best treatment option for them. If they have tried one triptan and it was not effective, or the side effects of the triptan were considerable, it may be helpful to try other triptans before moving to more expensive or invasive treatment options.
Paula Dumas of the Migraine World Summit asks: “People who might be at risk for medication overuse headache, or rebound: Are we finding that gepants are a better option for those folks?”
Dr. Dodick, director of the headache program at the Mayo Clinic in Arizona, responds:
“Yeah, that’s a great question. So, one of the key attributes of the gepants is that they may be the first, really the first, acute treatment for migraine that doesn’t cause medication overuse headache, or rebound. In fact — and maybe if you take a gepant every day, you actually drive the frequency down. So you’re going to see a medicine now that’s approved for acute treatment. … So people who have gotten into trouble before with rebound, from triptans, or opioids, or analgesics or whatever sort — these gepants, both in animals and now in humans, don’t seem to cause rebound or medication overuse headache.”8
Did you know?
Did you know that if none of the triptans provide effective relief for you, there are other new options available, such as ditans and gepants?
Triptans and Ditans
Ditans are a new class of drugs for the acute treatment of migraine. Ditans became available for use in the United States healthcare system in 2019. Both ditans and triptans work by blocking the release of CGRP, but unlike triptans, ditans do not dilate blood vessels. This makes ditans safer for people living with migraine and vascular diseases, such as cardiovascular disease, Raynaud’s syndrome, high blood pressure, diabetes, or stroke. Ditans are more expensive than triptans and are not as readily accessible in as many countries as triptans.10
Triptans and Gepants
Gepants are a new class of drugs for both the acute and preventive treatment of migraine attacks. This represents a recent breakthrough for migraine management. Gepants are CGRP antagonists that block CGRP receptor sites, but unlike triptans they do not constrict blood vessels or arteries. This makes gepants safe for people living with vascular diseases, such as cardiovascular conditions, Raynaud’s syndrome, high blood pressure, diabetes, or stroke. Gepants are more expensive than triptans and are not as readily accessible in as many healthcare systems worldwide as triptans.7
During their 2021 Migraine World Summit interview, Paula Dumas and Dr. David Dodick discuss geptans and how they differ from triptans.
Click here for their discussion
Dr. Dodick explains, “So gepants bind to that CGRP receptor on the trigeminal nerve and block the effect of CGRP. Triptans inhibit or suppress the release of it, whereas gepants block its ability to act because it gums up the receptor, if you will. That’s the difference. CGRP receptor antagonists, or gepants, bind to the blood vessel, but they dilate the blood vessel rather than constrict the blood vessel. So CGRP, when it binds to a blood vessel, dilates it.”11
Dumas says, “What I’m hearing you say is, they appear to be safer for people whohave either heart issues or a family history of heart problems.”
Dr. Dodick: “They appear to be because they don’t constrict blood vessels. And so,now, of course, we use them in people who do have cardiovascular disease, and they appear to be safe … And they’re not contraindicated in people who have had heart disease or stroke, and we’ve been using them in those patients and seemingly safely. So they’re an option for patients who can’t take triptans because of this cardiovascular risk. And because they work differently, they don’t have the same side effect profile. So, the most common side effects seen with the gepants — and in a very small number of patients in clinical trials — some had a little bit of fatigue, and some had a little bit of nausea, but 95% of the patients had no side effects — as opposed to triptans, where they have a completely different side effect profile. So far, we have a class of medicine where if a patient doesn’t respond to a triptan, can’t take a triptan, or has side effects from a triptan, this may be a reasonable option. And I should say, there’s data that supports that they can be effective in people who have failed triptans.”
In the video below, Dr. Dodick discusses the incredible significance of these new treatment options, both for patients and practitioners.
Triptans and Botox
OnabotulinumtoxinA, Botox, is a neurotoxin designed to block nerve stimulation and relax muscles.7 Injections are given in the face, head, and neck. Botox is available for people living with chronic migraine. Unlike triptans, Botox was not specifically designed for migraine treatment and does not target CGRP or blood vessels. However, many people find it an effective treatment to help prevent acute migraine attacks. Botox is accessible in most countries and is more expensive than triptans.
Triptans and Opiods
Opioids are a broad class of drugs that enhance pleasure and block pain receptor sites in the brain. They are most commonly used following surgery and for the treatment of chronic pain conditions. Opioids are not recommended for the treatment of migraine due to their addictive nature.
Drug-to-Drug Interactions23
Triptans with MAOIs
The enzyme monoamine oxidase (MAO) in MAOI antidepressants breaks down some or all of the following four triptans: almotriptan, rizatriptan, sumatriptan, and zomitriptan. Eletriptan, frovatriptan, and naratriptan, however, are not broken down by MAOIs and, therefore, are better options for people with migraine on MAOIs.
Triptans with SSRIs and SNRIs
People on triptans and an SSRI (serotonin reuptake inhibitor antidepressant) or SNRI (serotonin norepinephrine inhibitor antidepressant) run the risk of developing serotonin syndrome, since triptans and these antidepressants each affect serotonin levels. The rare condition can cause confusion; changes in blood pressure; increased heart rate and sweating; and muscle changes like twitching, jerking, and clumsiness. While serotonin syndrome is rare, it’s good to know about it, so it can be recognized and treated should it occur.
Triptans with Ergots
No large studies have been conducted to evaluate the effect, so the exact narrowing process is unknown, but ergots may constrict arteries, and triptans are estimated to constrict normal heart arteries by up to 20%. To avoid potentially harmful blood vessel narrowing, triptans and ergots are not to be taken on the same day.
The Bottom Line
Triptans are a class of drugs used to acutely treat migraine attacks. There are seven different types of triptans, and each works a little differently. If one triptan doesn’t work well for a person’s migraine attacks or the side effects of the triptan are considerable, another triptan may be tried and found to work better. While shown to be highly effective when taken early during an attack, and often considered a first-line migraine treatment, triptans are not a good fit for everyone. Medication overuse headache, MOH, or a history of cardiovascular disease are two reasons why doctors may choose a different medication, such as a gepant or ditan, instead of a triptan.
The landscape of medical treatment for migraine has evolved considerably over the years. It now offers a variety of medications to help alleviate acute attacks and prevent them in the future.
In this article you will learn more about the numerous medications offered to people with migraine today. It should allow you to easily prepare for your next doctor’s appointment, armed with knowledge.
The landscape of medical treatment for migraine has evolved considerably over the years. It now offers a variety of medications to help alleviate acute attacks and prevent them in the future.
In this article you will learn more about the numerous medications offered to people with migraine today. It should allow you to easily prepare for your next doctor’s appointment, armed with knowledge.
Acute Medication for Migraine Headache
When you are experiencing a migraine attack, acute medication can be taken to stop or minimize the intensity and duration of the pain as well as other migraine symptoms.
Acute medication for migraine includes a range of options, from simple pain relievers and nonsteroidal anti-inflammatory drugs (NSAIDs) used to treat pain in general, to triptans and gepants, which are specially developed to treat migraine.1
Acute medications are available in various forms, including oral pills, dissolvable tablets, nasal sprays, and injections. If you tend to vomit during migraine attacks, using nasal sprays or injections can help ensure that the medication remains in your system.
Achieving the Most Effective Acute Treatment
Most people who experience migraine attacks should consider acute medication. When effective, acute medication can significantly relieve attacks in either severity or duration, or both.
For the best possible effect, you should take your acute medication at the first sign of a migraine attack. Dr. Andrew Charles says that there have been multiple studies showing that treatment when pain is mild is beneficial.
“If you treat your migraine attacks when the pain is mild, studies show that there is a greater chance of reaching a pain-free endpoint, or pain relief within a certain period of time. In addition, the chance that an attack will recur is actually reduced,” says Dr. Charles.
Delays in taking acute medication can lead to increased pain, greater disability, and a more significant impact from the headache. The benchmark of an effective acute treatment is “back to function” within two hours of treatment.
In many cases, a combination of medications may be necessary to achieve adequate relief. However, do not mix medications on your own; these must be prescribed by your doctor.
When experiencing frequent migraine attacks, it can be challenging to avoid overusing acute medications. Using various types of medication, like over-the-counter pain relievers or triptans combined with NSAIDs for 10 days or more each month, can lead to medication overuse headache (MOH),2 also known as rebound headache. This can result in even more frequent migraine attacks and increased pain. You can read more about medication overuse headache and how to avoid it below.
Consider keeping a migraine diary to track your migraine attacks, what medication you use and its effects. There are several apps available for this purpose that you can download and easily access from your phone.
Different Types of Acute Migraine Medication
There are several different types of acute medication for migraine attacks. These include:
ditans
pain relievers (analgesics)
NSAIDs
triptans
ergotamine
gepants
First-Line Acute Treatments for Migraine
If you are experiencing mild to moderate migraine attacks, first-line acute treatment includes: pain relievers (analgesics). For example:10
aspirin (Bayer)
acetaminophen (Tylenol)
NSAIDs including ibuprofen (Advil)
If you are experiencing moderate to severe migraine attacks, first-line acute treatment includes:10
Triptans, including:
sumatriptan (Imitrex) — this is the triptan commonly prescribed before trying others.
zolmitriptan (Zomig)
eletriptan (Relpax)
rizatriptan (Maxalt)
almotriptan (Axert)
frovatriptan (Frova)
naratriptan (Amerge)
It may take awhile to find a medication that is effective and well tolerated. Up to three different triptans may be tried via various routes of administration before physicians will look to another class of drugs, including gepants and ditans.10 Gepants and ditans are also prescribed to individuals who are unable to take triptans since these newer drugs don’t constrict blood vessels.10
Ditans(selective 5HT1F receptor agonists) such as lasmiditan (Reyvow)
A New Drug on the Horizon
In January 2025 the FDA approved a new acute medication for migraine called Symbravo. Symbravo combines rizatriptan, a fast-acting triptan, and meloxicam, a long-lasting NSAID. It is designed to effectively relieve the most severe migraine symptoms quickly and maintain relief for a longer duration.12
Other Medications Available for the Acute Treatment of Migraine
Additional prescribed medications include ergotamine derivatives, such as dihydroergotamine (DHE). Many physicians also recommend treating migraine attacks with neuromodulation devices such as CEFALY and Nerivio (more on these below).
Also, if you experience nausea during your attacks, anti-nausea medication (antiemetics) can not only keep the acute medicine you take in your system but also enhance the absorption of it.
“Once people start getting nauseated, they’re much harder to treat. And we know that the gut is not working well in general during a migraine, even without nausea. Once people start getting nauseated, the likelihood of being able to swallow a pill, have it dissolved, have it be absorbed, and be effective, goes way down.”
Over-the counter (non-prescription) options in anti-nausea medication include dimenhydrinate (Dramamine) and diphenhydramine (Benadryl). Prescription antiemetics include metoclopramide (Reglan) and ondansetron (Zofran).
How to Know What Acute Medication to Take and When
According to Dr. Friedman, people living with migraine often have different kinds of attacks. Treatments should not only be tailored to each individual patient, but also to their specific type(s) of attacks.
“Share with your doctor the typical timeframe of a migraine attack, from when you first become aware of an attack, to then when the pain starts. How long does it take for your medication to work? Does the headache come back? What percentage of the time is your acute medication effective? This information may help you to get a better acute treatment plan,” Dr. Friedman explains.
How to Avoid Medication Overuse Headache (MOH)
Medication overuse headache (MOH) is a type of headache that occurs from using too much medication for an existing headache disorder, like migraine, and is common among individuals with 15 or more headache days per month.3 Medication overuse headache can occur when using various types of medication, like over-the-counter pain relievers or triptans combined with NSAIDs, for 10 days or more each month.4
Adding preventive methods to reduce headache frequency is important to prevent medication overuse headache. Another strategy to avoid medication overuse headache is to use gepants for preventive and/or acute treatment. Gepants have not been shown to contribute to medication overuse headache unlike other acute treatments.5
Preventive Medication for Migraine
The primary goal of preventive medication for migraine is to lessen the impact of the condition by reducing either the frequency or severity of migraine attacks — or both.
Preventive medication includes a range of options. These include antidepressants, beta blockers, calcium channel blockers, anti-seizure medications and Botox. There are also preventive medications developed especially for migraine, such as Calcitonin Gene Related Peptides (CGRP) monoclonal antibodies.
The medication comes in various forms, including oral pills, injections, and intravenous (IV) drugs. Successful preventive treatment for migraines is measured by its ability to reduce the disease burden and improve quality of life.
When to Start Using Preventive Medication for Migraine
Effective preventive migraine treatment starts with an accurate diagnosis, which may involve ruling out other potential causes of your symptoms. Whether or not you should take preventive medication depends on the number of migraine attacks you experience per month and how much they affect your daily life.
Practitioners suggest starting migraine preventive drug therapy when one or more of the following conditions is present:11
You have more than three migraine attacks or at least eight headache days in one month.
You have severe, debilitating headache attacks despite acute treatment.
You have contraindications to acute medication or can’t tolerate its side effects.
You have medication overuse headache.
You have hemiplegic migraine, basilar migraine, or migraine with prolonged aura.
You prefer to go on a preventive treatment.
Tips to Find Your Most Effective Migraine Prevention
Don’t get discouraged if the first medication you try doesn’t have the desired effect. Finding a preventive medication that works for you may require some trial and error.
Different preventive medications can complement each other, and you might need to use more than one.
Keep a migraine diary to track your attacks, symptoms, and the effects of treatments.
An effective preventive treatment is typically defined by a 50% reduction in the frequency or severity of attacks.
If your doctor tells you they’ve tried everything or run out of options, it may be time to consider another doctor. There are many options and strategies to consider for someone who knows how to treat patients with migraine disorder.
Different Types of Preventive Migraine Medication
First-Line Treatments for Migraine Prevention
Options include:
Anti-seizure medication (anticonvulsants), including divalproex (Depakote) and topiramate (Topamax)
Blood pressure lowering medication, including beta blockers, such as propranolol (Hemangeol); also, calcium channel blockers, such as verapamil (Verelan)
Other Approved Treatments for Migraine Prevention9
Antidepressants, such as amitriptyline (Elavil)
Gepants, including rimegepant (Nurtec ODT) and atogepant (Qulipta)
Calcitonin Gene Related Peptides (CGRP) monoclonal antibodies (mAbs), for example: erenumab (Aimovig), galcanezumab (Emgality), fremanezumab (Ajovy), and eptinezumab (Vyepti)
OnabotuliniumtoxinA (Botox)
Due to comorbidities, other conditions you may have in addition to migraine, certain preventive medications may be better than others for you.9 For instance, calcium channel blockers may be preferred if you have dizziness or vertigo. If you have insomnia and/or depression, a tricyclic antidepressant may be chosen for you.
Neuromodulation Devices for Migraine
How Neuromodulation Devices Work
Neuromodulation devices, sometimes referred to as nerve stimulation devices or neurostimulation devices, modulate the activity of different nerves such as the occipital nerve, trigeminal nerve, vagus nerve, and the supraorbital and supratrochlear nerves in the forehead. Some neuromodulation devices are used for preventive treatment, some for acute treatment, and some have both options. These devices typically require a prescription.
When to Try Neuromodulation Devices
If you experience side effects from medication (Neuromodulation devices have limited side effects because they are not absorbed in the body.)
If you are in need of using acute medication more than 10 days a month
If you are under 18 (Some neuromodulation devices are approved for adolescents.)
Food and Drug Administration (FDA)-Approved Neuromodulation Devices for Migraine:8
If you are living with migraine and it is negatively impacting your life, it is recommended that you consult a headache specialist or a neurologist. You may experience difficulty in finding or getting in to see a headache specialist, as they are in short supply. Keep in mind that neurologists aren’t necessarily headache specialists, but they tend to treat a lot of patients with migraine.
Ensuring that your treatment is specifically tailored to address both acute attacks and preventive care is crucial. Various types of medications, both acute and preventive, work well together. Consider keeping a migraine journal to track the effects of different medications.
Additionally, consider non-drug therapies such as neuromodulation devices, chiropractic care, cognitive behavioral therapy (CBT), and lifestyle changes like regular exercise and consistent sleep routines.
Supplements to Consider
Supplements are another class of treatment that often comes up when talking about migraine.
Dr. Alexander Mauskop, director and founder of the New York Headache Center, and a board-certified neurologist and headache specialist, explains which supplements he would typically recommend for those living with migraine.
“If we don’t have any blood work to help us determine what supplements to use, we would first recommend magnesium because it has the most scientific evidence, and about 50% of people are deficient in magnesium. Second, the most proven supplement would be coenzyme Q10. We have a very large study looking at 1,550 people with migraine, and fully one third is deficient in CoQ10. My next recommendation would be a vitamin B2 — riboflavin. And then we also recommend herbal products such as feverfew. Another herbal supplement that I recommend is boswellia — frankincense.”
Improvement: What to Expect
For those living with frequent migraine attacks, any form of relief, whether small or significant, is greatly appreciated. However, according to Dr. Stewart J. Tepper, professor of neurology, people often settle for less than they should.
“I’m never satisfied until people are really not having any disability or impact from their migraines, and their function across all aspects of their life is back to normal,” says Dr. Tepper.
“If somebody has a very good response to a subcutaneous monoclonal antibody, but is still having a migraine attack or two per week, where previously they might have had 20 headache days in a month, it’s a pretty dramatic improvement for that person. But it may not be as good as they can get.”
Dr. Tepper suggests multiple ways to get an even greater drop in headache days, and improvement in quality of life.
“One way is to move from a subcutaneous injection of a monoclonal antibody once a month to an intravenous monoclonal antibody, and even move to the highest dose of that intravenous monoclonal antibody. Another option is to add onabotulinumtoxinA, or Botox. Sometimes the combination of the two will have an additive, or a synergistic effect,” says Dr. Tepper. He adds, “We can also consider a switch to the daily or every-other-day oral medications and combining gepants. All of these offer opportunities for people to do even better.”
Summary: Medication for Migraine Headaches
Medication for migraine headaches includes both acute and preventive medication. Most people with migraine should consider acute medication to effectively stop migraine attacks.
If you are experiencing migraine attacks four or more days per month, you can talk to your doctor about preventive treatment. If you are severely burdened by your migraine attacks, two a month is enough to consider preventive medication. See the full list of recommendations under the section When to Start Using Preventive Medications for Migraine.
It’s important to use a migraine diary to track migraine attacks, symptoms, and the effects of treatments used. Above all, remember the process takes time. Finding the right treatment, both acute and preventive, is often a process of trial and error. Don’t lose faith that there is treatment out there that will be able to help you.
Headaches are a shared experience impacting people across all walks of life. Those experiencing them move along and manage the best they can, tapping formal and informal supports, trying a spectrum of remedies, and taking one day at a time.
Headaches are a shared experience impacting people across all walks of life. Those experiencing them move along and manage the best they can, tapping formal and informal supports, trying a spectrum of remedies, and taking one day at a time.
However, there exists an elusive, complex, and problematic level of headache … the severe headache. This is a whole different ball game warranting further discussion since severe headaches can and do have a significant impact on those experiencing them.
This article dives into several Migraine World Summit interviews with renowned headache experts. They will explain what severe headaches are, their causes, and, most importantly, when and how to get help. Khalil Gibran once said, “Your pain is the breaking of the shell that encloses your understanding.” This touches deeply on managing a severe headache, where the struggle may bring insight and resilience. This information aims to help people living with and managing severe headache conditions feel more informed, empowered, and safe.
Common Causes of Severe Headache
What is a severe headache? Differing definitions and assumptions exist. It may be surprising to know severe headaches do not often occur in isolation, nor are they the main instigator. Also, many health conditions and headache variations fall under the severe headache spectrum (i.e. primary and secondary headache). Below are medical diagnoses where severe headache is a foundational component:
Common Diagnoses Featuring Severe Headache
Migraine Headache
This presents as throbbing pain, usually on one side of the head, often with nausea, vomiting, and sensitivity to light, smells and sound.
Cluster Headache
This headache type brings severe, burning, or piercing pain, usually around one eye, in clusters or cycles.
Sinus Headache
Sinus inflammation causes deep, constant pain in the forehead, cheekbones, or nose bridge.
Tension Headache
This tight, band-like head pain is often linked to stress or muscle strain.
Thunderclap Headache
This sudden, severe headache peaks within seconds to minutes and is often a sign of a more serious condition (e.g., subarachnoid hemorrhage).
Medication Overuse Headache
Frequent use of headache medication leads to daily/chronic headaches. Find more information on this in the next section.
Brain Tumor
A rare and growing tumor results in severe headache and other neurological symptoms.
Brain Injury/Post-Traumatic Headache
This severe headache follows a head injury or concussion.
Aneurysm
Bulging blood vessels in the brain cause sudden, severe head pain if they leak or rupture.
Infections
Infections such as meningitis, encephalitis, or an abscess can cause severe headache, fever, and neck stiffness.
Stroke
Severe headache and nerve, spinal cord, or brain function problems can be symptoms.
Cervicogenic Headache
Cervical spine/neck issues cause severe pain in the head and neck area.
Temporal Arteritis
Inflammation of blood vessels in the scalp leads to severe headache with tenderness in the temple(s).
Trigeminal Neuralgia
Irritation of the trigeminal nerve causes severe facial pain, sometimes perceived as a severe headache.
Hypertension
Extremely high blood pressure can often lead to what is described as pulsating head pain.
Carbon Monoxide Poisoning
Exposure to carbon monoxide gas can cause severe, throbbing head pain, with symptoms like dizziness and confusion.
Hangover
Severe headaches can occur after excessive alcohol consumption.
Eyestrain
Prolonged use of digital screens or uncorrected vision problems can lead to severe head pain.
Dehydration
Severe head pain can come from losing fluids in the body to the point of bodily function impairment.
Avoiding Medication Overuse Headache
As mentioned in the table above, overuse of medications, especially over-the-counter or prescription pain relievers, can lead to a headache returning as the medication wears off, creating a cycle of dependency and constant head pain. These are commonly referred to as rebound headaches.
During the Migraine World Summit’s 2016 event, Dr. Alan Rapoport stated, “They can hurt their liver. They can hurt their kidneys. What I’m interested in is it’ll hurt their [headache] because they’ll end up having more [headache], and the stuff will stop working on them, and they come in and say to me, ‘I keep taking this medicine, and my headache is still bothering me even more,’ and, again, they don’t understand that they’re actually unintentionally contributing to the headache.”1 Additionally, some medications targeting various other conditions (e.g., blood pressure or hormones) can trigger headache as a side effect.2
Dr. Gisela Terwindt explains what medications can cause medication overuse headache, as well as approaches to treatment.
Symptoms of Severe Headache
To understand severe headache it is important to identify unique symptoms. This includes intensity of pain, associated symptoms, as well as duration and frequency.3
Pain Intensity and Location
Pain intensity and location can vary greatly depending on the headache type. For example, migraine attacks can cause intense, throbbing pain on one side of the head. At the same time, a tension-type headache is typically constant, dull aching around the forehead or back of the head and neck. On the other hand, cluster headache involves excruciating pain, usually around one eye or side of the head, in cyclical time patterns.
Associated Symptoms
Accompanying symptoms of severe headache often include nausea, vomiting, sensitivity to light (photophobia), sensitivity to sound (phonophobia), and visual disturbances (aura). These travel alongside the headache pain, providing clues to the headache type. For example, migraine attacks frequently involve these additional symptoms. At the same time, cluster headache attacks can cause eye redness and tearing on the affected side. For other severe headache, such as thunderclap headache, other less-known associated symptoms can exist, such as speech difficulties, dizziness, seizures, confusion, vision changes, numbness, etc.4
Duration and Frequency
How long and how often head pain occurs assists in diagnosis. Migraine typically lasts several hours or days and may occur once in a while (episodic) to at least half of the month (chronic). Cluster headaches are often short, intense episodes lasting but minutes, occurring multiple times a day over weeks or months.
Another severe headache type is the thunderclap headache, which is sudden and severe, reaching maximum intensity within 60 seconds, and lasting at least five minutes. Additionally, hemicrania continua headache, which features persistent and unilateral pain that fluctuates in intensity but never fully disappears, is often accompanied by autonomic symptoms, disruptions to automatic functions. One can start to see how complex understanding and treating headache is since there are several combinations related to headache duration and frequency.
When a Serious Headache Requires Immediate Attention
When is a headache sufficiently serious to warrant outside help? While many times a headache can be treated at home, specific symptoms signal the need for urgent medical support. Recognizing these red flags is critical to avoid serious health complications.
One tool that can help identify these warning signs is the SNNOOP10 tool, a clinical guide used by healthcare providers in assessing headache symptoms. The SNNOOP10 tool covers areas such as:
Systemic symptoms (i.e., affecting the whole body, such as fever or weight loss)
Occurrence with positional changes (i.e., when you stand up or move around)
Onset during pregnancy
Previous headache history
Plus 10 other signs highlighting underlying conditions such as infection, vascular disorders, or structural brain issues.5
A tool like this can help you tell the difference between a typical headache and one that might indicate a life-threatening condition. The following are some key warning signs, which align with the SNNOOP10 criteria, indicating a headache may require immediate attention by a healthcare provider.6
Sudden Onset of Severe Headache
Imagine a headache that appears to come out of nowhere, and you would describe it as the worst headache of your life. For example, a pain so agonizing and disorienting that it causes you to pass out. These sudden and intense headaches can signal more critical conditions like the ones discussed earlier (e.g., subarachnoid hemorrhage from an aneurysm rupture). These types of headaches often quickly worsen and require immediate medical attention, as they can be life-threatening.
Headache with Neurological Symptoms
Imagine experiencing an intense headache but also slurring your words or noticing a side of your face drooping. As stated before, a headache accompanied by neurological symptoms (e.g., vision changes, speech difficulties, weakness, numbness, and seizures) could suggest a possible underlying, serious problem impacting the brain, such as a stroke or brain tumor. Time-sensitive evaluation by a healthcare professional is recommended when these symptoms occur.
Headache After a Head Injury
If a headache persists or worsens following a concussion/head injury, other problems may be involved (e.g., brain swelling or bleeding). That’s especially so if the head pain is accompanied by confusion, dizziness, vomiting, or changes in alertness. For example, imagine having a head injury and initially feeling fine. But then, you start experiencing a relentless, worsening headache. You might become more irritable, light-headed, and confused. Prompt medical assessment is needed to rule out serious injuries.
Persistent or Worsening Headache
Envision experiencing a headache for several weeks. Still, the pain has become sharper and more intense without relief from regular painkillers. You might also start feeling nauseous to the point of vomiting. Over time, a constant or worsening headache can be a sign of severe conditions (e.g., a brain tumor or a build-up of fluid in the brain’s ventricles). A headache that transitions from mild to severe and does not stop needs a more thorough investigation.
Headache with Fever or Stiff Neck
Severe headache, fever, and stiff neck can sometimes signal an infection. Meningitis, for example, is an infection of the membranes around the brain and spinal cord. An individual with meningitis might become sensitive to light and develop a rash, fever, and pounding headache.7This mix of symptoms requires immediate medical intervention to prevent severe, possibly life-threatening complications.
Mental Health Considerations
Severe headache can have a significant impact on mental health, contributing to anxiety, depression, and an overall reduced quality of life. If you experience a daily headache, you might feel trapped by your pain. Over time, you may withdraw from social activities and become increasingly anxious about the next attack. Persistent pain and discomfort can lead to emotional distress, irritability, and difficulty concentrating — further exacerbating mental health challenges. This ongoing struggle can leave you feeling hopeless and frustrated, making it essential to seek support.
At the 2018 Migraine World Summit, Dr. Dawn Buse discussed migraine and two of its common comorbidities, anxiety and depression. She shared, “They are their little evil team of three. I’m thinking of the arch-villains in a comic book with these three. In research, we have noticed that when we can treat any one of them, the others get better. If we just reduce headache days somewhat, migraine, depression, and anxiety get better.”8
Access to support networks and professional guidance can help you manage pain and provide coping strategies, fostering resilience and improving mental and physical well-being.
Diagnosis and Medical Evaluation
Where to Go for Care
Immediate consultation (at an emergency room) is crucial if your headache is sudden and intense, accompanied by neurological symptoms, or follows a head injury. For persistent or worsening headaches, regular visits to your general physician or neurologist can help identify and manage underlying causes. So, what happens when someone reaches out for help in dealing with severe head pain?
Diagnostic Tests and Procedures (CT Scan, MRI, etc.)
To determine the cause of severe headache, health professionals may recommend various tests and procedures. Tests like CT scans and MRIs can reveal issues in the brain that might be causing pain. Blood tests check for infections or other underlying conditions. In some cases, a lumbar puncture (i.e., spinal tap) can rule out conditions such as meningitis or a subarachnoid hemorrhage.9
Importance of an Accurate Diagnosis
An accurate diagnosis is necessary for effective treatment and management of severe headache, and identifying underlying causes. Whether the head pain is due to migraine, cluster headache, or potentially life-threatening conditions like a brain tumor or aneurysm, understanding the exact cause allows for strategic treatment, quality of life improvement, and prevention of further issues.
This is not always a straightforward or smooth process. Sometimes, you must self-advocate and be assertive when navigating the complex web of healthcare systems. Joe Coe from the Global Healthy Living Foundation emphasizes this: “If you feel like you’re going to be shamed or questioned about who you are as a person, you’re not going to live that indignity and seek care. We know that people are delaying treatment to routine wellness visits because their primary care physician isn’t affirming of their identity or sexual orientation.”10
How Tracking Health Data Helps
For an accurate diagnosis, doctors gather detailed health information. Be prepared to track important data and answer questions about themes discussed in this article, such as:
Onset, duration, and frequency of headache
Associated symptoms like nausea, light sensitivity, or aura
Medical history, including any past head injuries, family history of headache, and current medications/treatments
Potential triggers
These clues help doctors paint an accurate picture (e.g., type of headache, more serious conditions, etc.) and develop a holistic treatment plan tailored to your needs. For instance, noting if your head pain worsens after physical exertion or specific stressors can guide more targeted testing.
Also, by tracking your symptoms (in a diary or tracking app like Migraine Buddy), you can capture insights consistently, improving communication and navigation within the healthcare system and enhancing the chances of an accurate diagnosis. This also allows you to better understand your condition and recognize potential triggers or patterns, leading to improved lifestyle management.
Preventing Strategies: A Balanced Approach
While certain severe headache conditions like migraine and cluster headache may have specific triggers, prevention often comes down to maintaining a healthy, balanced lifestyle. For headache caused by other factors, such as tumors, the best we can do is stay as healthy as possible. Although some individuals may experience a severe headache despite being in good health, adopting a balanced lifestyle can enhance recovery and management of these conditions. For more insights on managing severe chronic headache conditions, check out a related article here.
Summary
A severe headache isn’t just an inconvenience. It can profoundly impact your life and well-being. This article provides an overview of the complexities of severe headache, exploring various causes, triggers, and associated conditions. Recognizing warning signs and understanding when to get help early can prevent serious complications. Gaining a better understanding of severe headache conditions allows for making more informed decisions about your health, improving your quality of life, and helping you navigate the challenges that come with severe head pain.
Resources and References
Links to outside organizations and articles are provided for informational purposes only and imply no endorsement on behalf of the Migraine World Summit.
Further Reading
International Headache Society. (2018). The international classification of headache disorders, 3rd edition (ICHD-3). Cephalalgia, 38(1), 1-211. https://www.ichd-3.org/
Migraine World Summit: gathers leading headache experts from around the world to share the latest research, treatments, and strategies for managing migraine. The summit offers extensive video interviews, articles, and resources for individuals dealing with migraine.
European Headache Federation (EHF): provides educational resources, conducts research, and collaborates with other organizations to enhance understanding and treatment of headache.
Migraine Trust (UK): offers a wealth of resources including information on treatments, support groups, and advocacy for people living with migraine. They also conduct and support research initiatives focused on migraine.
American Migraine Foundation (AMF): provides comprehensive resources, including educational materials, research updates, and support networks for those living with migraine. Their global outreach includes webinars and community support initiatives.
Migraine Canada: offers educational resources, treatment information, and a community forum for individuals suffering from migraine. They also collaborate with international organizations to enhance migraine awareness and research.
International Association for the Study of Pain (IASP): promotes the study of pain, including headache. They provide resources for both professionals and patients, host international conferences, and support global pain research.
The World Federation of Neurology (WFN) – Headache Group: focused on improving the care and management of headache globally. They offer educational resources and guidelines, and promote research in the field of headache disorders.
Global Patient Advocacy Coalition (GPAC): advocates for patients with chronic pain conditions, including migraine, on an international scale. They work to influence global health policies and provide resources and support for patients and caregivers.
According to the World Health Organization (WHO), headache disorders are among some of the most common nervous system disorders, and around 15% of the world’s population experiences migraine attacks.19 It’s estimated that up to 5% of people diagnosed with migraine meet the criteria for chronic migraine: having a headache at least 15 days per month, with at least eight of those days featuring migraine symptoms, for over three months.
According to the World Health Organization (WHO), headache disorders are among some of the most common nervous system disorders, and around 15% of the world’s population experiences migraine attacks.19It’s estimated that up to 5% of people diagnosed with migraine meet the criteria for chronic migraine: having a headache at least 15 days per month, with at least eight of those days featuring migraine symptoms, for over three months.
While there are various preventive medications for chronic migraine on the market, many come with a host of side effects, making them uncomfortable or undesirable. Of these preventives, Botox injections typically come without systemic side effects and do not require a daily or even monthly dose. Botox has been shown to be an effective preventive medication for chronic migraine, with over a million people receiving treatment as of 2023.
If you’ve been wondering about Botox treatment for chronic migraine, read on for a primer on this popular treatment, and get prepared for your next doctor’s appointment.
What is Botox?
Botox comes from the toxin onabotulinumtoxinA, produced by the bacteria Clostridium botulinum. The pharmaceutical company Allergan, owned by AbbVie, treats and purifies this botulinum toxin to create a protein that, when injected, stops muscle contractions. It does this by interfering with the release of neurotransmitters at the neuromuscular junction, where the nerves and muscles meet.9 This interrupts the pain pathway. Once the protein is created, the dose is calculated and put into vials containing 100 or 200 units, and it is called Botox.
History of Botox as Treatment for Chronic Migraine
Botox is commonly associated with cosmetic use, which minimizes facial wrinkles and fine lines. While cosmetic use accounts for half of all Botox treatments, it has also been used as a medical treatment for various conditions besides migraine, such as strabismus (crossed eyes), since the 1970s.
Botox Medical Treatments
Condition
Symptoms
Cervical Dystonia
severe neck and muscle spasms
Blepharospasm
eye twitch
Hyperhidrosis
severe and excessive sweating
Strabismus
misaligned/crossed eyes
Bruxism
grinding of teeth
Overactive Bladder
urge to urinate that’s difficult to control
Chronic Migraine
for over three months, having 15 or more headache days per month, 8 of which feature migraine symptoms
In 1998, Beverly Hills cosmetic surgeon Dr. William Binder documented that several patients who received Botox on their foreheads and around their eyes reported improved migraine attacks. This led to several scientific studies centered on Botox’s potential for treating migraine. For example, the PREEMPT study, ending in 2008, resulted in Botox being FDA-approved in the United States for the prevention of chronic migraine in 2010.3 Botox was also approved for migraine prevention by the Medicines and Healthcare Products Regulatory Agency (MHRA) in the United Kingdom that year.6 The Therapeutic Goods Administration (TGA) in Australia quickly followed suit with its formal approval of Botox for chronic migraine in 2011.1
Dr. Andrew Blumenfeld further explains the research conducted that led to Botox being approved for chronic migraine.
How Botox Helps Prevent Migraine Attacks
Botox is used differently depending on the condition being treated. Receiving treatment for one condition will not necessarily affect another condition. Dr. Andrew Blumenfeld, a primary researcher in the PREEMPT clinical trial, says that Botox is injected shallowly into the muscle at “31 dedicated injection sites, all of which are around pain fibers … since these sites are at sensory nerve-ending sites, they won’t have the effect as if injected into cosmetic sites.”
The PREEMPT clinical trial produced the injection site locations and eventually led to the FDA approval of Botox as a migraine preventive treatment. The purpose of injecting at these sites is to suppress the peripheral pain nerves connecting the brain with painful stimuli involved in migraine. Since the mechanisms of migraine are complex and not fully understood, it is hard to fully understand what makes Botox work.
Often, a person with migraine will try to control their triggers to minimize the number of episodes. However, many individuals with migraine are easily triggered by everyday things that are often unavoidable, such as a glare, loud environment, or strong smell. Botox decreases this hypersensitization and allows for better control of environmental triggers.
Dr. Karl Ng, director of the Headache Clinic at Royal North Shore Hospital, further explains the complexity of migraine and the importance of helping patients get relief when triggers are difficult or impossible to avoid.
The pathophysiology of migraine is complex, but the treatment of migraine may be broken down fairly broadly into several categories. First of all, a good history should be taken, not just to identify what the problem is, and that the patient satisfies the criteria for migraine, but also to see if there are any precipitants, so are there any triggers that the patient has. This may take many different forms, be it stress, or lack of sleep, or even certain foods. If those things can be avoided first off, then that should be the focus. However, some people can’t avoid these things, and, therefore, we have to look for other ways of trying to help them.
Figuring Out if Botox is a Good Fit
For 30 years, researchers have been searching for biomarkers indicating whether Botox will be successful for individual patients.15 While more research is needed to say who specifically will benefit from Botox, several factors can indicate that it may not be the correct preventive medication for some.
Episodic migraine is not currently considered a good fit for Botox; this is because the injection sites developed during the PREEMPT study were found while focusing on individuals with chronic migraine with a stable headache history.3
Individuals who have had a craniotomy, or skull surgery, should inform their provider. If a person has an implanted stimulator in their scalp, the injector must know where to avoid damaging the leads.10
Botox should be avoided if there is an infection at the proposed injection site or if the individual is hypersensitive to any botulinum toxin preparation.12
Of the PREEMPT study, Dr. Blumenfeld states, “We typically saw a 50% response rate. This means that the study participant felt 50% better.” One in four study participants saw a 75% response rate. Participants also frequently noted dramatic improvement in their neck and shoulder pain. Many of the physicians who spoke with the Migraine World Summit have seen even better results among their patients than those of the PREEMPT Trial.13 Their reported results were sometimes as good as 75% of patients expressing a marked decrease in headache days and migraine attacks.
The FDA recommends repeating Botox every 12 weeks. However, 44-62.9% of patients who receive Botox to treat their chronic migraine report noticing a wearing off around weeks 9-10.15 Some patients have benefitted from a shortened time window between injection sessions.
Getting Access to Botox Treatment for Migraine
Insurance Requirements
Access to Botox through insurance companies involves several administrative hurdles before being considered. First, an individual must meet the FDA standards for chronic migraine.7 This includes each attack lasting at least four hours per day. Many insurance companies in the U.S., as well as the U.K.’s National Institute for Health and Care Excellence (N.I.C.E.), require the person with migraine to try two to three different classes of preventive treatment without seeing results.8 Frequently, insurance companies will then need prior authorization for the treatment, which must be updated every year.
While Botox may be considered an expensive preventive option, Botox can be cost-saving compared to emergency room visits, urgent care visits, imaging studies, or other medication costs. It does not take many emergency room visits to pay for Botox treatment. Getting approved for migraine preventive treatment with Botox can be challenging and time-consuming, but the option may be a viable one for many.
One thing to note: Many insurance companies will deny Botox if a patient already uses a CGRP medication. This differs across the healthcare industry. It is recommended that you speak to your insurance company to get their criteria.
There is a Botox savings program in the United States for those with commercial insurance. This program helps cover some of the costs of the medication and procedure. It is designed to help cover the out-of-pocket costs after insurance.
Finding the Right Physician
Finding the right physician to administer Botox is crucial to getting good results from Botox for chronic migraine. Ideally, look for a headache specialist or neurologist who has been specifically trained in the use of Botox for chronic migraine. A dermatologist or cosmetic surgeon focused on cosmetics would not place the injections at the nerve sites needed to treat chronic migraine. A good place to start is Allergan’s search tool for finding a Botox Specialist. It links to physicians who are experienced in treating chronic migraines with Botox.
Before undergoing preventive treatment with Botox, ask questions such as:
Does the provider inject the full 31 injection sites?
What dose does the provider use?
How many patients has the provider treated for chronic migraine?
Have their patients experienced drooping eyelids or neck pain?
What percentage of patients decides to continue the preventive treatment?
How Botox Treatment Feels
Choosing Botox can be scary, as people fear the pain of repeatedly getting injected in the head and neck. While no injection is entirely comfortable, going into the appointment with informed expectations can help ease the fear.
The needles used for Botox are slightly thicker than an acupuncture needle and about half an inch long. With both the small needles and the injection’s shallowness, some say it feels like a very fast pinch with some sting. The Botox administrator usually uses conversation as a distraction; for most, this is enough for the injection to go unnoticed.
The exception is usually when the patient is in a pain flare, perhaps during an active migraine attack or allodynia. Since the pain structures of the head and neck are already hypersensitive, the injections can cause more discomfort, with some patients describing it as similar to a bee sting. While the discomfort usually passes quickly, here are a few things that can help mitigate some of this discomfort:
Take Tylenol before the appointment.
Ask for a local anesthetic.
Use ice to numb the injection sites before and after the injection.
Potential Side Effects
In a conversation with the Migraine World Summit, Dr. Bronwyn Jenkins discussed the most common side effects of Botox. “The most common is minor skin irritation, such as redness, a small bump at the injection site, and some bruising. Flu-like symptoms, such as fatigue, chills, and muscle stiffness, have also been reported.” These side effects usually fade within a few days of onset.
Difficulty lifting eyebrows, droopy eyelids (less than 3%)
Headache, neck stiffness, and muscle spasms (4%)
Discomfort in the neck muscles (9%)
Many of these side effects are short-lived, and having a well-trained Botox administrator can minimize many of them.
There are some very rare and severe effects of Botox such as: difficulty swallowing, speaking, or breathing. This can be due to weakening of associated muscles, can be severe and result in loss of life. You are at the highest risk if these problems are preexisting before injection. Swallowing problems may last for several months.
There is also the risk of the Botox toxin spreading to surrounding tissues after the treatment. This can lead to: loss of strength and all-over muscle weakness, double vision, blurred vision, drooping eyelids, hoarseness or change or loss of voice, trouble saying words clearly, loss of bladder control, trouble breathing, and trouble swallowing.12
Safety Considerations and Misconceptions
Since Botox has become widely known and accepted, there are a few myths and fears that many have when considering Botox for treating migraine. These include:
1. Botox is a toxin produced by the Clostridium botulinum bacteria. Is it possible to get botulism from getting Botox?
When Dr. Blumenfeld discussed these concerns with the Migraine World Summit, he shared, “To get sick with botulism from Botox, a person would need to be injected with around 3,000 units of Botox. Botox is put into 100- to 200-unit bottles by Abbvie. Botox, when used to treat chronic migraine, is usually around 155 units. Due to the large difference in units, it would be almost impossible to get botulism from Botox accidentally.”
2. What happens if the injection protocol is not followed?
The injection protocol for using Botox to treat migraine is vital for success. If the provider does not administer the full 31 sites, the treatment may be less effective, and the adverse side effects will usually increase.
3. What if the injection is too deep or too large?
Having Botox injected too deeply into the muscle under the skin can cause weakness and pain in the muscle. For example, if the injection is placed too deep into the muscles of the neck, then there may be pain or difficulty holding the head up. This is why having a skilled administrator is essential. Botox should be injected superficially in the correct location and with the proper doses to get the desired reduction in migraine attacks.
4. Is Botox safe during pregnancy and breastfeeding?
There is currently not enough research to say if Botox is safe during pregnancy and breastfeeding. There have been studies on the effect of Botox exposure before the patient is aware of the pregnancy. These studies show the rate of fetal birth defects in these cases at the same rate as is seen in the general population.5 However, Botox has been less researched during the second and third trimesters. It is best to talk to your Botox provider about pregnancy if this is a concern.4
5. There is also a misconception that it will take about nine months of Botox treatment to see an effect.
Botox has a cumulative effect; it can take up to 10 months to get the full results, but many start feeling relief after two to three weeks.
The Bottom Line
Botox is considered a safe and effective migraine preventive option for many. Due to its high success rates, it has proven popular with both patients and providers. With over a million people with chronic migraine having received Botox, it is safe to say that Botox is a preventive option that deserves more attention.
Migraine disease can be debilitating and often difficult to manage. It can present as many different types and vary in symptoms, frequency (from episodic to chronic), and intensity. Learning if you have migraine in the first place, and, second, what type you have, can help guide you to the appropriate health care provider and a constructive treatment plan.
Introduction
Migraine disease can be debilitating and often difficult to manage. It can present as many different types and vary in symptoms, frequency (from episodic to chronic), and intensity. Learning if you have migraine in the first place, and, second, what type you have, can help guide you to the appropriate health care provider and a constructive treatment plan.
Not Sure If You Have a Migraine Disorder?
Below is a screening tool to help you determine if what you are experiencing is migraine.
Screening Tool: Headache vs. Migraine
Migraine vs. Tension-Type Headache
Migraine is more than just a headache. It is a neurological (related to the brain) disorder influenced by genetic and environmental factors. It can include symptoms such as light or noise sensitivity, nausea, vomiting, dizziness, stomach pain, brain fog, and much more. Together, these symptoms form what practitioners call a migraine “attack,” which can interfere with a person’s daily activities and significantly disrupt their way of life.
“So we know the diagnostic criteria for migraine, which is one-sided pain, throbbing pain, moderate to severe pain, pain that worsens with routine activity, plus one of the following: either nausea or vomiting, or light or sound sensitivity. But when we talk about tension-type headache, it’s the opposite.7
Dr. Newman further explains tension-type headache: “It’s pain on both sides of the head, it’s non-throbbing pain, it’s mild or moderate pain, and it’s not disabling. And in clinical practice, doctors who treat people with headache look at it as a headache without any associated features. It’s just the head pain.”1
Migraine
Tension Headache
Head Pain Location
Often One-Sided
Always Bilateral
Intensity
Moderate to Severe, Disabling
Mild to Moderate
Duration
4-72 Hours
30 minutes-1 day
Symptoms
Headache; Sensitivity to Light, Sounds, and Smells; Nausea; Fatigue; Brain Fog and More
Head Pain
Watch or listen to Dr. David Dodick, professor emeritus at the Mayo Clinic, further describe what is happening in the brain during a migraine attack.
Migraine Statistics
Migraine occurs in both children and adults.
Migraine is 3X more common in women than in men.
Migraine is more common than diabetes, epilepsy, and asthma combined.
Migraine affects more than a billion people globally and is the second most common cause of years of disability.2
Approximately 50% of migraine disease is linked to genetics, the other 50% to environmental factors.
Most individuals with migraine have a family history of the disease.
Individuals with underlying medical conditions such as epilepsy, sleep disorders, and mood disorders are more likely to develop migraine disease.
The Different Migraine Types
Migraine With Aura (Classic Migraine)
Migraine with aura, also known as classic migraine, is a type of migraine where a person experiences a “warning sign,” or aura, before the actual head pain begins. Aura can present visually in the form of seeing flashing lights or zigzag patterns. Auras may also bring speech disturbances; numbness, tingling or weakness in the body; nausea; loss of appetite; confusion; blurred vision; mood changes; and fatigue. This often coincides with increased sensitivity to light, noise, or sound.
Most aura symptoms are reversible and resolve within an hour. The most common aura symptoms are visual disturbances, which can last up to 60 minutes and then settle. Anyone who experiences an aura that lasts over an hour should seek immediate medical care, in order to rule out something more serious.3
Migraine without aura, also known as common migraine, is a type of migraine with moderate to severe episodes of head pain without aura symptoms. Head pain can be on one side or both, and is usually worse with physical activity. This form is a more frequent type of migraine and occurs without warning. It can include symptoms like nausea, vomiting, confusion, blurred vision, mood changes, fatigue, and increased sensitivity to sound, light, or noise.
Chronic Migraine
The International Headache Society defines chronic migraine as experiencing headache on 15 or more days per month for more than three months, where at least eight of those headache days have migraine features. Again, those features include things like nausea, vomiting, sensitivity to light or sound, and moderate to severe headache that is described as throbbing or pulsing.
It is estimated that 3-5% of the U.S. population experiences chronic migraine.4 Further statistics show 2.5 out of 100 episodic migraine patients will develop chronic migraine.
Menstrual Migraine and Menstrually Related Migraine
Characteristics
These migraine attacks start 2-3 days before a woman’s period to the 3rd day of menstrual flow.
For women with migraine, 60% report their attacks occur at the same time as their menstrual cycle.
Menstrual migraine attacks are more severe and lengthier than attacks during other times of the month.
These attacks are caused by a rapid drop in estrogen levels, which occurs right before a period.
This type can be challenging to treat and sometimes doesn’t respond to typical migraine therapies.
Menstrually related migraine occurs when patients have both menstrual migraine and another type of migraine, like migraine with aura, occurring at other times during the month.5
Vestibular Migraine (Migraine-Associated Vertigo)
Vestibular Migraine is a migraine type in which the prominent symptom is vertigo or dizziness. Individuals with vestibular migraine describe this as a sensation of rocking back and forth, spinning, moving while their body is still — or a sudden dropping sensation while sitting still. Patients with vestibular migraine don’t always have a headache with their migraine attack; however, they usually have other migraine symptoms like light or sound sensitivity and nausea. Some vestibular patients have a history of motion sickness or sensitivity beginning in childhood. In adults, vestibular migraine is the second most common cause of vertigo.6 To take a more extensive look at vestibular migraine, explore our in-depth article on this migraine type.
“… I am looking at you now, and looking at my room, but imagine you feel that you’re really looking at the world from about a foot or two behind where you are — an out-of-body displacement. We call that ‘Alice in Wonderland’ syndrome. Those are symptoms that generate from abnormalities of [the] processing of normal vestibular information in the brain that comes from the inner ears.”7
Abdominal Migraine
Abdominal migraine is a type of migraine in which the patient experiences episodic, central abdominal pain along with other features of migraine. These can include nausea, vomiting, loss of appetite, and a pale complexion in the face. This type usually starts in childhood, with the average onset at age 7, but it can occur in adults, typically with a family history of migraine. Abdominal migraine is more common in girls than boys. Most people with abdominal migraine feel well between attacks.8
By their teenage years, 60% of kids who experienced abdominal migraine will outgrow their abdominal pain. Yet up to 70% of those with abdominal migraine can develop typical migraine as adults. To learn more about abdominal migraine, check out our in-depth look at this migraine type.
Hemiplegic Migraine
This is a rare form of migraine that along with other migraine symptoms includes weakness on one side of the body (hemiplegia). People with hemiplegic migraine may or may not have head pain during their attacks. Symptoms can last from hours to days. This type of migraine often begins in childhood and runs in families. Hemiplegic migraine can present like a stroke, so it is important to be evaluated by a healthcare provider to get a clear diagnosis through testing and imaging studies.9
Dr. Stephen Silberstein discussed this rare form of migraine at the Migraine World Summit:
“There are two types of hemiplegic migraine. One is the type that’s genetic and runs in families, which means you have a relative with it. The second type is (what) we call sporadic hemiplegic migraine, which means you don’t have a first-degree relative with it. Hemiplegic migraine is really defined by the fact that during the aura, or the neurological symptoms that precede the migraine attack, the patient is weak on one side of the body.”10
Migraine With Brainstem Aura (Formerly Basilar-Type Migraine)
Ten percent of people who experience migraine with aura will be diagnosed with migraine with brainstem aura. Individuals that have migraine with brainstem aura may also deal with vertigo, dizziness, slurred speech, ringing in the ears, and double vision. These symptoms develop gradually from the area in the brain called the brainstem and can happen before or during a typical migraine headache. Migraine with brainstem aura usually occurs during adulthood; however, it can occur at any age. Features can also include disorientation or confusion as well as temporary loss of consciousness, which is known as syncope.11
“The reason we called it migraine with brainstem aura is because of the symptoms that these patients have. They have double vision. They slur their speech, like they’ve had too much to drink. They’re unsteady on their feet. They have vertigo. Sometimes they have numbness and tingling, but on both sides of the body.12
Retinal Migraine
Characteristics
These attacks cause temporary loss of vision in one eye and are followed by a headache within an hour.
The loss of vision is reversible.
This form is most common in women of childbearing years.
Vision loss can last up to anywhere between 5-60 minutes.
This typically occurs in one eye.
Retinal migraine is a rare type of migraine and often confused with ocular migraine. Headache specialists now use migraine with aura interchangeably to describe ocular migraine.
Other issues with the eye should be ruled out before retinal migraine is diagnosed.13
Migraine Aura Without Headache (Formerly Known as Silent Migraine or Acephalgic Migraine)
Experts refer to this type as a migraine attack with aura but no headache pain. It is a rare type and is currently known as migraine aura without headache. Only 3-4% of patients with migraine have migraine aura without headache. An individual’s, often debilitating, aura can include temporary language, speech, and visual disturbances — typically lasting for under an hour. Individuals can be triggered by typical migraine triggers and often experience other types of migraine as well. Treatment for individuals with migraine aura without headache can be extremely challenging.14
Status Migrainosus or Status Migraine
Status migrainosus, or status migraine, is a type of migraine where an attack can last for days or weeks and does not respond to treatment. This migraine type is one of the most difficult to treat. Individuals with status migraine have a history of migraine, either migraine with or without aura. People with chronic migraine, obesity, lower socioeconomic status, lack of access to quality healthcare, and struggles with mental health are at higher risk of status migraine. It is also thought that individuals who have migraine disorder but are not on a preventive migraine medication are more at risk.
Allow Christina Treppendahl, FNP-BC, AWH, MHD, to explain status migraine biology.
“ … you get this peripheral sensitization at first, with something that triggers a migraine. You get peripheral sensitization, and that’s outside the central nervous system. And then the neurons in the meninges send signals to your deep brain to kind of have an autoplay of more pain, more pain, more pain, more pain. And so you get into what we call this central sensitization, where the brain does not know how to shut that off.”15
Summary
Understanding the different types of migraine can be overwhelming initially. The first and crucial step to healing is often finding the correct diagnosis. Regardless of migraine type, finding the appropriate healthcare provider can be instrumental in receiving the best migraine treatments for you. If possible, it is important to seek out a headache specialist, or neurologist who regularly treats migraines, for evaluation and treatment. Working with a specialist will reveal the many migraine treatment options and therapies that can assist you while living with migraine.
The Migraine World Summit is here to help. Visit our website to find links to provider directories and migraine support groups. The Migraine World Summit can help educate you and give you the power to improve your quality of life one step at a time.
Links to outside organizations and articles are provided for informational purposes only and imply no endorsement on behalf of the Migraine World Summit.